Preventative spending in Scotland
This briefing explores prevention as a principle of public service delivery which includes risk avoidance and mitigation, long-term thinking, and linking spending and outcomes. The briefing includes an overview of challenges with implementation of prevention, international examples and summaries of interviews with subject experts.
Disclaimer
This briefing paper was prepared by Ota Dvorak during his internship with SPICe as part of the UKRI Policy Internship scheme. The internship was supervised by SPICe Senior Researcher Ailsa Burn-Murdoch.
This briefing paper provides a snapshot of the work being done to explore prevention in public services in Scotland and elsewhere, the aim being to inform, highlight relevant sources of further information, and present a discourse on the topic of prevention.
It should be noted that although some parts of this briefing might look like qualitative analysis, this is not an exhaustive review of all available literature and data and no structured analysis was conducted for the production of this briefing. Stakeholder interviews were conducted on an informal basis, and should not be considered to be the official standpoints of any organisations mentioned in this briefing paper.
As with all guest publications, the findings and conclusions of this briefing are the views of the author at the time of publication and not those of SPICe, or of the Scottish Parliament.
Summary
During the last couple of decades, western countries have been feeling the effects of a change in the demographic composition of their populations. People are living longer, fewer are being born, and this had led to ageing populations. Having an older population, especially one with a high proportion of people above the age of 65, places higher demands on public services like healthcare and social care. In 2022, one in five people in Scotland were aged 65 and over. Combined with the increased demand for public health services during and after the COVID-19 pandemic, this demographic shift has presented a challenge for providers of public services.
Independent and Government-funded studies have pointed to the deteriorating quality and rising cost of various public services. Scottish healthcare providers and local authorities, who provide social care and other services, rely on funding from the Scottish Government, and are at serious risk of not being able to fulfil their statutory duties due to pressure on budgets. Experts have issued warnings that the financial situation of public services is not sustainable, and are projecting that problems will get worse. There is urgent need for reform of public services, which the Scottish Government has recognised.
One potential way to do this would be to reorient services in a way that encourages them to direct more resources towards preventative approaches. Based on an amalgamation of other definitions of prevention, we propose the following definition:
A preventative action aims as a primary goal to reduce an individual's or a population's demand for urgent, reactive public services now and in the future, by removing risk factors, increasing resilience to risk factors, or providing early identification or intervention.
Preventative approaches are built around removing as many risk factors from people's lives as possible whilst supporting people to be strong and resilient to any remaining risk factors, and working with people to identify any issues as soon as possible and act swiftly. This way of working contrasts with a traditional reactive system where public service providers treat people who come to them with a problem.
It might seem logical to try and prevent problems instead of treating their symptoms, to invest in health and wellbeing rather than in treating illness, however it is not so simple. Many think that there are systematic barriers, which are holding back preventative reform. These include the ways in which resources are allocated by the Government, which splits the budget by Portfolio rather than by outcome, or a lack of clarity on what prevention would specifically look like, how much it would cost, and what benefits it would bring.
The Scottish Government has been working to try and implement preventative principles into Scottish policy with recent publications like the Public Service Reform Strategy (June 2025) or the National Performance Framework (new version in draft as of February 2026). So far, many written commitments have been made, but little data and detail has been shared, despite requests from Scottish Parliament committees. The Scottish Government has stated that by late-2026 it expects to finish a pilot project on preventative spend across the Scottish Budget. This aims to enable the Government to create a baseline understanding of how much money is currently being spent on prevention in Scotland, and in which sector it is being spent. It remains to be seen how the results of this pilot might influence further action from the Government.
In this briefing, we explain some of the factors which have contributed to the challenging situation that public services find themselves in. The briefing then sets out the characteristics which might determine whether a person will need public services, and at which point in their life. We then present definitions of prevention and introduce some of the underlying principles behind a prevention-based public service system. We go on to explain the current systematic hurdles in implementing this system. A number of the Scottish Parliament's committees have undertaken scrutiny relating to prevention in Session 6 of the Scottish Parliament. There is also a large quantity of work being done on the topic of prevention by the Scottish Government, as well as independent think tanks and other organisations. We present some of this work in this report, but it's important to note that this is a fast evolving field of research and practice. We also set out some examples of novel resource allocation methods used in various other countries to enable more consideration of the long-term scenarios and linking resources to outcomes. To produce this briefing, we spoke to experts from various organisations and we have included summaries of our talks with them.
The intention of this briefing is to serve as a first port of call for someone looking to get familiar with prevention as a delivery model for public services. We encourage the reader to follow links presented here to learn more detail and to follow up with the various organisations we mention throughout the briefing to find out about their latest work on this topic. We would remind the reader that while a lot of the work discussed is focused on healthcare, prevention goes beyond the healthcare sector, and the principles can be used in any setting within the public or private sector. Prevention is not just vaccinations and hard hats, it is about having a pre-emptive, risk-minimising, and strength-building mindset.
A perfect storm?
The Scottish Fiscal Commission (SFC) in its February 2026 Fiscal Sustainability Perspectives report warned of a potential multi-billion gap between funding and spending on day-to-day public services, which may impact as soon as 2029-301 . Scottish Household Survey results show a declining satisfaction with public services2. Public health outcomes, like life expectancy at birth, are no longer improving3.
This situation is not unique to Scotland, many countries in Europe and globally are struggling with similar challenges. Countries which provide a high level of public services. are finding themselves in a situation where, over the past decades, economic growth has failed to meet predictions, the number of people who pay taxes has either decreased or stayed the same, the population has aged, and the demand for public services has soared. This perfect storm of public service delivery creates increasing requirements for short-term spending on "front-line services", which can make it more difficult to allocate resources towards long-term goals, especially in cases where institutional rigidity is preventing change.
In this chapter, we explore how this problem came to be and look at some of the symptoms of struggling public services. Throughout this briefing, we refer to "public services" a lot. Unless further specified, by this we mean devolved public services in Scotland like healthcare, social care, education, or public transport. In some cases, we look at a specific service in more detail. We encourage the reader to think about prevention in the context of all public services, not just healthcare.
Demographic change
The demographics of a population will determine the type and volume of public services the population will require. A population with a high proportion of children aged 4-16 may require more funding for public schools, while a population with a high proportion of older people would likely need more money for healthcare.
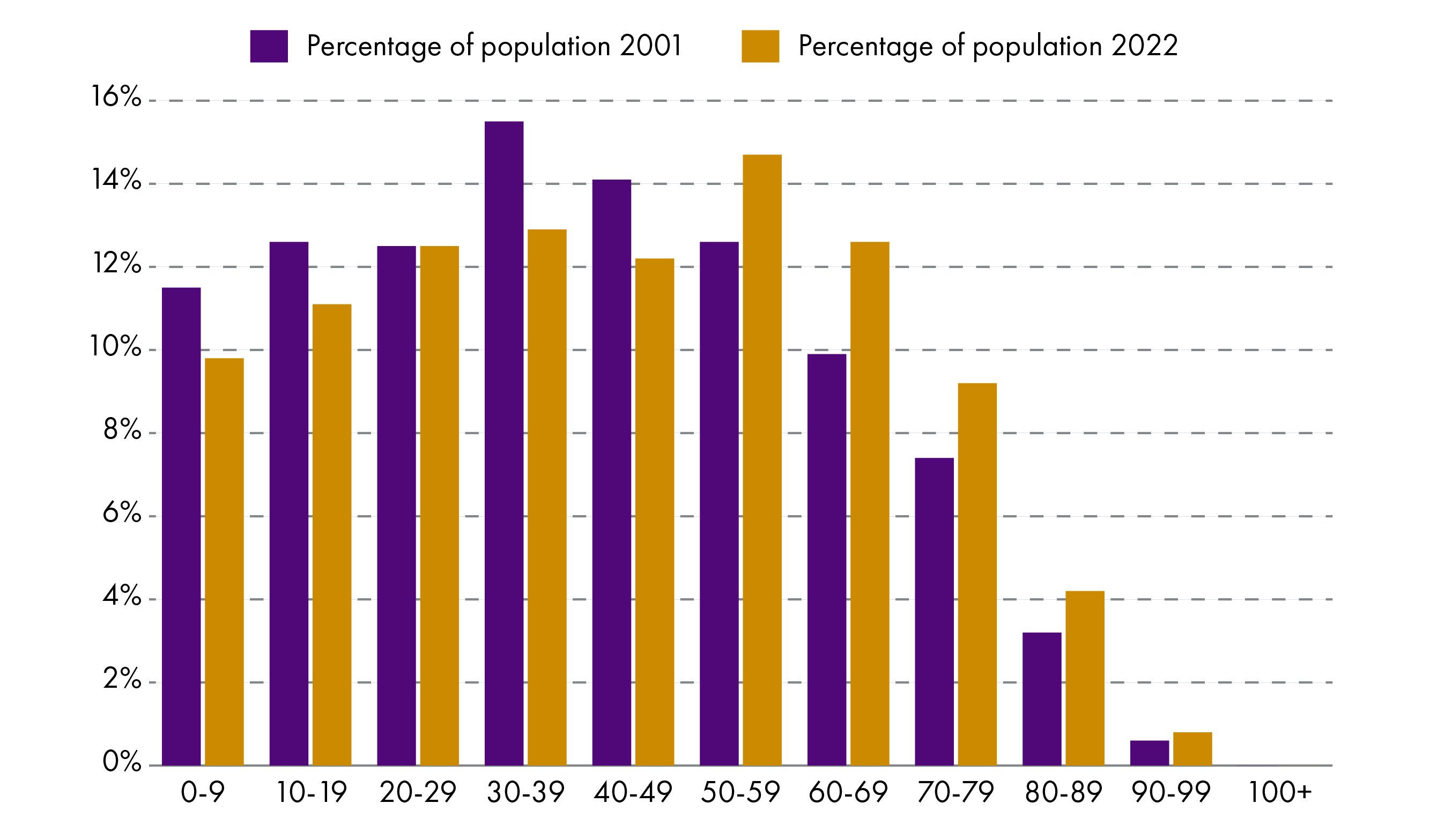
Data from Scotland's census 2001 (Table UV4 - Age by single year), and Scotland's census 2022 (Table UV103 - Age by single year).
Between 1971 and 2021, the average number of children born to each woman in Scotland fell from 2.5 to 1.311, meanwhile the life expectancy increased from around 70 to 79 over the same time 2. Put simply, people are living longer, and fewer are being born. This leads to a change in population structure – the average age of the population is increasing. Figure 1 uses Scottish census data to show how the population structure by age group changed between 2001 and 2022. The proportion of people above the age of 65 increased from 15.9% to 20%, while the proportion of people between the ages 16 and 65 decreased from 64.9% to 63.6%. Note that we extrapolate the Scottish life expectancy for 1971 from data for England and Wales for 19713.
The median age shifted from 39 to 42 in just two decades (2001 to 2022). Within that time, the proportion of people who self-reported as not being in good health in the Scottish Census had more than doubled, from 10% in 2001, to 21% 2022. In the 2001 census, this is the percentage of population reporting to be in “not good health”. In the 2022 census, this shows the percentage of the population reporting to be in “fair”, “bad”, or “very bad” health.
Taken together, these statistics show that over time the proportion of older people in the population has grown, the percentage of the population of working age has decreased, and more people report being in poor health. This presents challenges for the delivery of public services.
Age, healthcare, and taxes
The public service needs of individuals change throughout our lives. Here we use the example of healthcare, because it is the largest portion of public service spending. Typically, we need quite a lot of health care as babies, then not so much during most of adulthood, but when we reach 60 our demand for health care starts to increase.
Figure 2 shows a forecast profile of healthcare spending costs in 2029-30 by patient age group (in 2024-25 prices). Annual health care costs start rising steeply once a person reaches 60. Between the 2001 and 2022 census counts, the number of people aged 60 or more living in Scotland increased by 37%, suggesting that there is now a higher proportion of people who need more expensive healthcare than there was at the turn of the century.
Using the Scottish Census data shown in Figure 1 and multiplying it by the annual healthcare cost by patient age from Figure 2, we can estimate that, using the same prices of health care per patient of a given age, providing the same levels of healthcare for Scotland in 2022 may have cost £3 billion more than in 2001. This is an average increase of 10% per person. That is before taking into account inflationary changes to the cost of delivering services, or any changes in the type of services delivered.
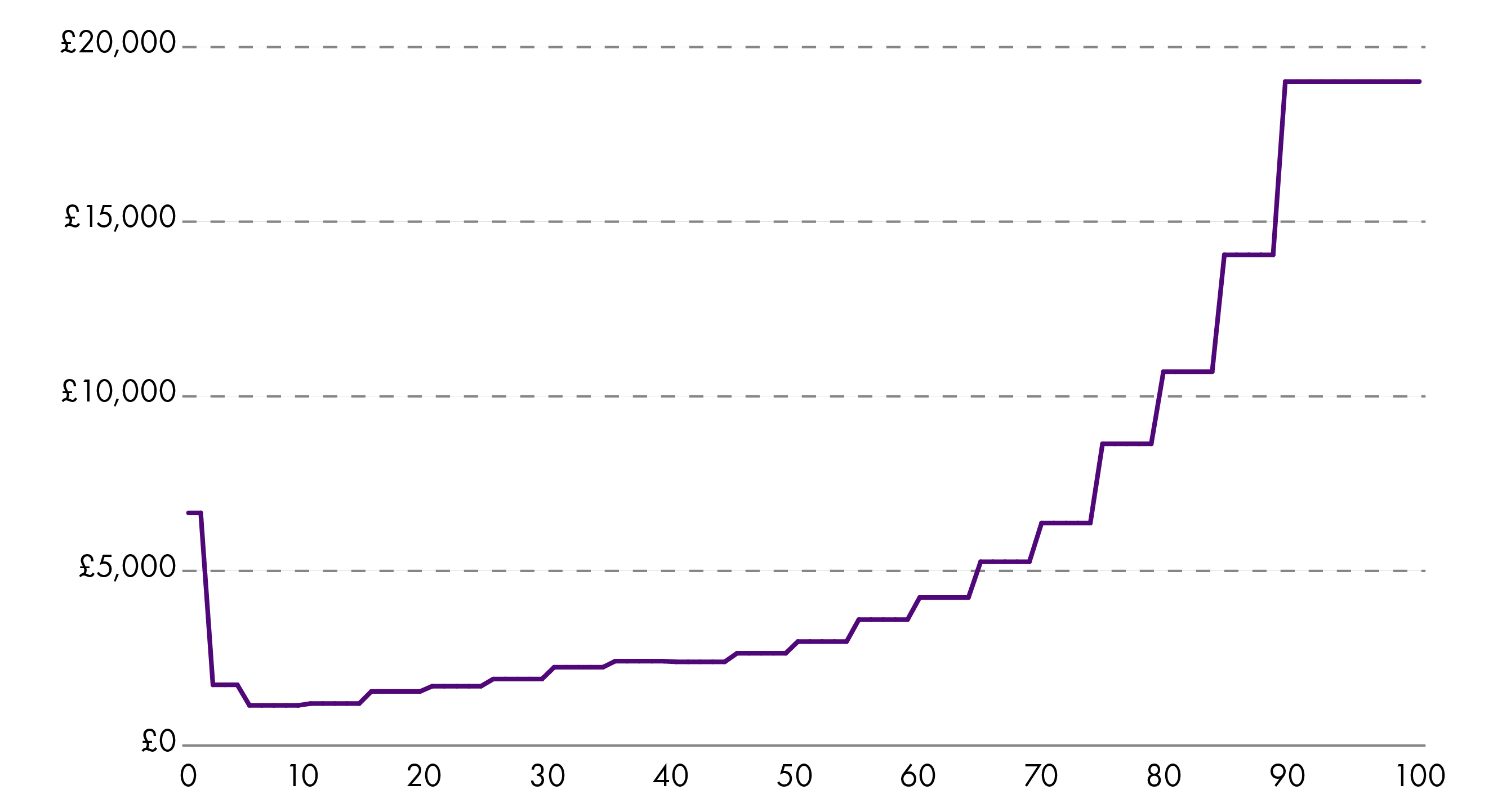
Data adapted from SFC's Fiscal sustainability report 2025, originally collected by SFC from Public Health Scotland, the NHS, and the Office for Budget Responsibility. Data averaged across males and females.
During the same time, based on Scottish Census data, the proportion of the Scottish population aged 16-64 decreased and, whilst more people were economically active, this was a modest increase compared to the increase in the proportion of the population who were retired or self-reported as being in poor health. Being "economically active" refers to people in full-time or part-time employment, self-employed, unemployed (but seeking employment), and to full-time students. Table 1 shows some selected differences between the Scottish population in 2001 and 2022.
| Population characteristic | 2001 | 2022 |
|---|---|---|
| Median age | 39 | 42 |
| % of population aged 65 and over | 16% | 20% |
| % of population aged 80 and over | 4% | 5% |
| % of population aged 16-64 | 65% | 64% |
| % of population not in good health | 10% | 21% |
| % of population who are economically active | 48% | 54% |
| % of population who are retired | 10% | 19% |
Scottish Census data. Percentages show the proportion of the 2001 and 2022 population respectively.
This changes how much tax income the Scottish Government can collect in order to finance public services like healthcare. Figure 3 shows how the mean income by age group (closely linked to amount taxable per person) peaks between 40-49 years, then sharply drops off above 60. The highest proportion of jobs are also worked by people in their forties than people in any other age group. A population with more people in the 60+ age bracket will be able to contribute less tax income compared to a younger population, which impacts on the funding available for public services.
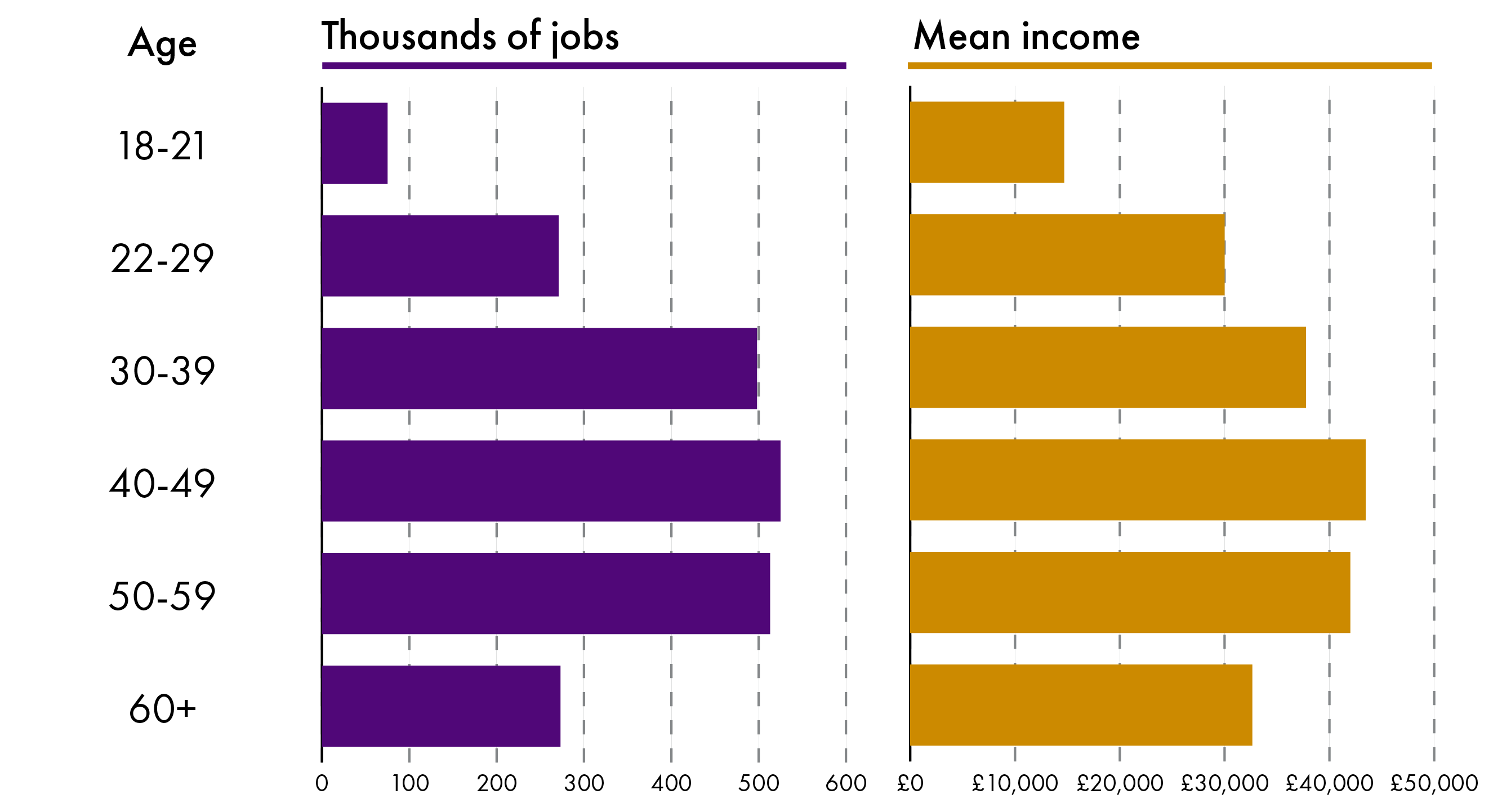
Data from the Office for National Statistics Earnings and hours worked, UK region by age group dataset (Data set PROV - Work Region Age Table WGOR Age.7a Annual pay - Gross 2025, Section S92000003).
In summary, Scotland's population has aged, which has implications beyond more expensive healthcare and a likelihood of lower income tax collection. This is backed up by spending data - 63% of the Scottish adult social care expenditure in 2018-19 went towards services for older people1. Spending on State Pensions and Pension Credit also increases with a higher percentage of the population being above the State Pension age. In the next section we look at how Scottish public services are coping with this challenge.
Public services facing multiple challenges
The demographic change we've explored has been compounded with a large public service demand spike during and following the COVID-19 pandemic. This has created an unprecedented demand for public services in Scotland and, despite record budget allocations, service providers are struggling to balance their budgets. Over the past six years, seven NHS boards in Scotland had to ask for a total of £500 million in 'brokerage' (loans to enable them to balance their budgets)1. But achieving financial balance is not the only problem that public service providers face. In this section, we talk about the broader financial issues they face, people's satisfaction with the services, and life expectancy.
The change in demographic was in part brought by an increase in life expectancy – one of the key measures of population health2. This presents a bit of a paradox: an increase in life expectancy is a symptom of good public services, but it also creates a challenging situation for these services, who now have to serve an older demographic with higher healthcare needs.
Life expectancy is one area we can explore as a measure of population health. Since the 1980s, life expectancy in Scotland and in the UK has gradually increased until the 2010s, but since then, it has plateaued3.
Throughout this time, life expectancy in Scotland has lagged behind that of the UK as a whole by roughly two years, as shown in Figure 4. Public Health Scotland (PHS), in its latest 10-year strategy report, identified that life expectancy in Scotland is the lowest out of all UK countries4, and below the average across member countries of the Organisation for Economic Co-operation and Development (OECD). Figure 4 shows a comparison of life expectancy between Switzerland (the highest of all OECD countries), Mexico (the lowest of all OECD countries), the UK, the OECD average, and Scotland. Using life expectancy as a measure of population health tells us that Scotland's population health has stagnated for the past fifteen or so years, and that it has underperformed compared to both the rest of the UK, and the OECD average.
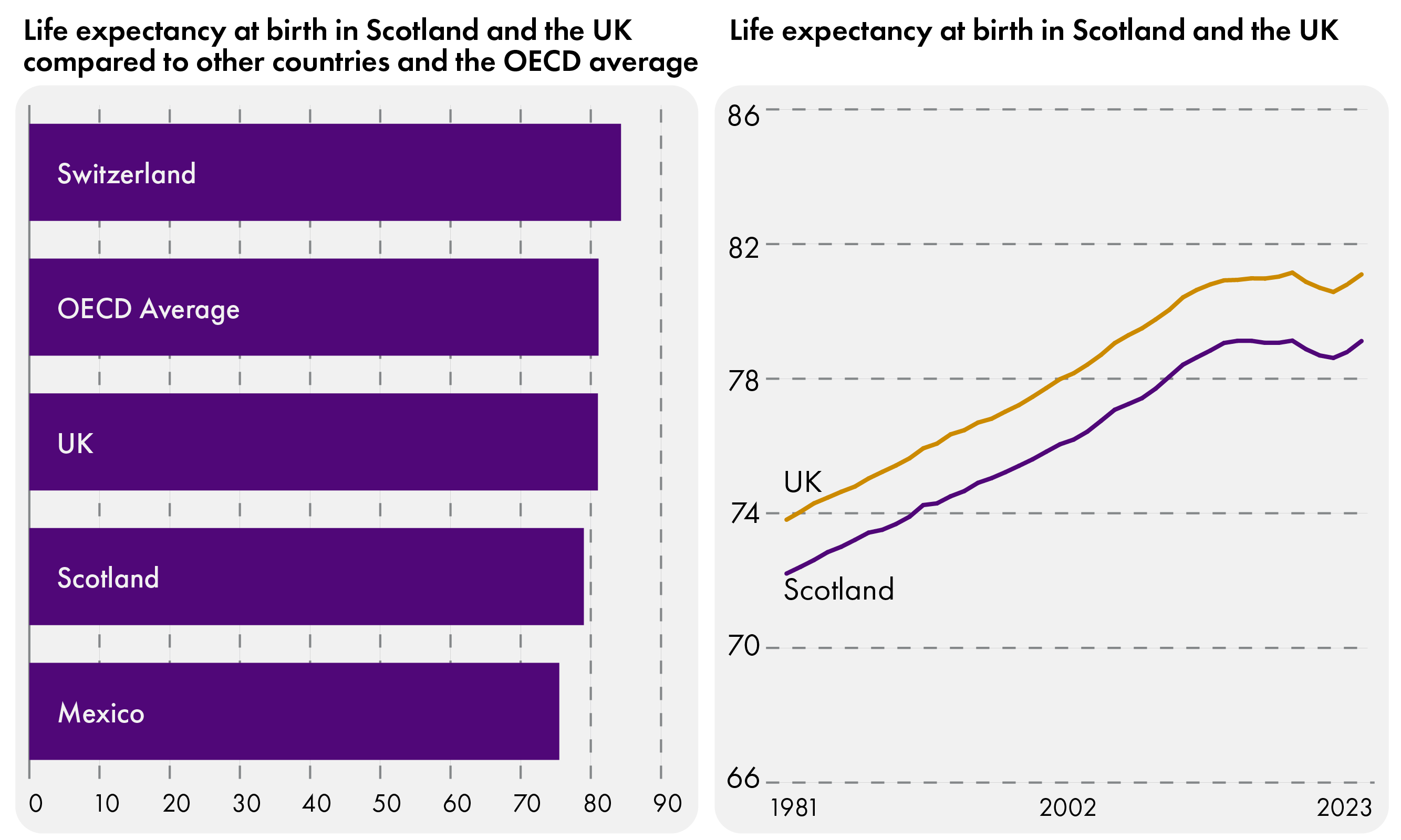
Left - Data from PHS report Together we can: Our 10-year strategy to 2035 and the OECD data explorer (Life expectancy dataset), Right - Office for National Statistics Published data related to life expectancies (National life tables: UK and Scotland), Where required data was averaged between males and females.
At the same time, budget allocations for healthcare providers have risen, and the SFC forecasts that they will keep growing. The Scottish health and social care sector, already the largest area of devolved spending, received its highest allocation ever in the 2026-27 Scottish Budget, beating the record set the previous year. SFC's predictions show that health and social care spending may reach 55% of the Scottish devolved budget by 2074-75, and that spending will exceed funding by at least 4% (and potentially up to 11.1%) over the coming decades5.
There is nothing new about rising costs of public services. A 1944 Edinburgh Evening News article laments the £66,000 year on year increase in teachers’ salaries and public assistance, which the Edinburgh Town Council would have to match from rates levied6. Scottish Councils increased Council Tax rates again in early 2026, reflecting increased pressure on budgets alongside a need to carry out their statutory duties.
Despite a third of Scottish devolved spending going towards health and social care, the public report being less and less satisfied with the delivery of public services, as shown in Figure 57. Critically, when comparing this against data from the Scottish Index of Multiple Deprivation (SIMD), we can notice how satisfaction changed differently for people living in the 20% least deprived areas of Scotland (Quintile 5) and for those living in the 20% most deprived (Quintile 1). In 2013, those in Quntile 1 were the most satisfied, followed by Quintile 2, and the others broadly similar. In 2023, Satisfaction was lowest among Quintile 4 (41% satisfied with all three categories of public services measured - healthcare, education, public transport) and highest among Quintile 5 (47%), but the greatest fall in satisfaction levels came in Quintile 1 (from 64% in 2013 to 42% satisfied in 2023).
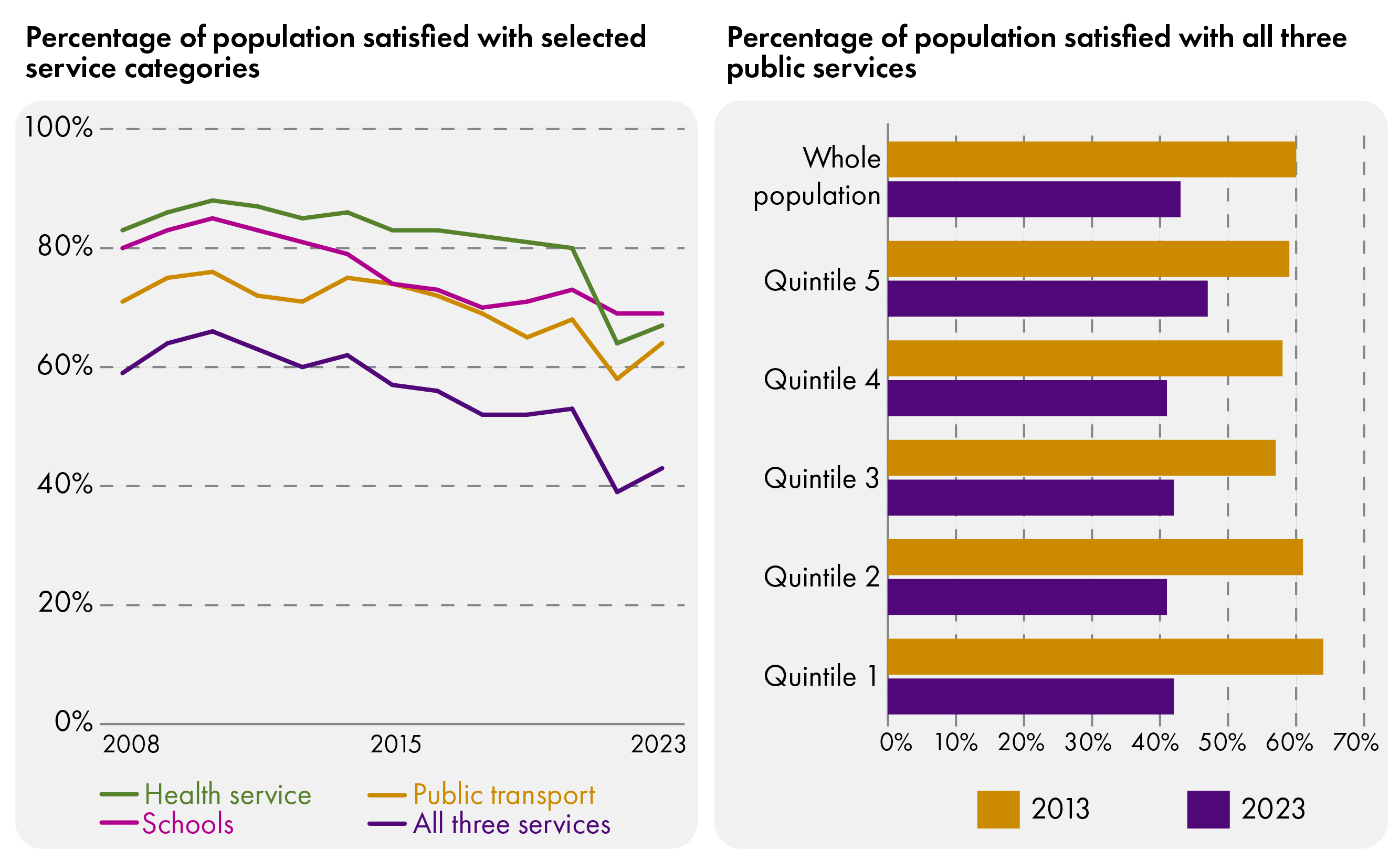
Data from the Scottish Household Survey Data Explorer (Left - Tables 6.1, 6.5, 6.9, and 6.13 for years 2008-2023, Right - Table 6.15 for years 2013 and 2023).
In 2011, the Christie Commission published a Report on the future delivery of public services, in which Dr Campbell Christie urged the Scottish Government to “act quickly and decisively” and said it was“essential that the Scottish Government exercises its leadership by initiating a fundamental public service reform process”. The report contained sobering predictions about the fiscal outlook beyond the 2011 Scottish Spending Review: “It is not easy to predict beyond 2014-15 and it is not easy to be optimistic.”. The key themes identified by the Commission are still relevant 15 years on. The Commission said:
High levels of public resources are devoted annually to alleviating social problems and tackling ‘failure demand’ – demand which could have been avoided by earlier preventative measures
Until now we have funded that ‘failure demand’ with annually increasing budgets. That is no longer an option. So tackling these fundamental inequalities has to be a key objective of public service reform.
[The Commission] takes a positive view of public services and stresses the importance of a virtuous cycle between improving the delivery and effectiveness of public services and fostering stronger and more balanced economic development.
The most significant challenge to sustainable services is the likely and considerable escalation in demand in the longer term.
Our analysis suggests that responses to these challenges must include taking demand out of the system through preventative actions and early intervention to tackle the root causes of inequality and negative outcomes…
The Commission's concern for the outlook past 2014-15 turned out to be justified, even if it could not have predicted the COVID-19 pandemic. Between 2014-15 and 2024-25, health spending increased by 24.9% in real terms8. In the latest Finance and Performance review of the Scottish NHS by Audit Scotland, the auditors paint a bleak picture of the current situation:
Even with increased funding, the NHS in Scotland is not in a financially sustainable position. NHS boards did achieve unprecedented levels of savings. But boards are still struggling to break even, with seven territorial boards requiring Scottish Government loans.
Audit Scotland highlights that these Scottish Government loans are not being repaid, with only £7 million out of the total £500 million of emergency funding these boards received over the previous six years1 having been repaid at the point of publication. Audit Scotland has also flagged the issues around the future (and current) sustainability of delivery of public services in its Transforming health and social care in Scotland hub. A January 2026 report explained how delayed hospital discharges are a symptom of these issues.
In the Integration Joint Boards Financial Bulletin 2024-25 (February 2026) Audit Scotland warned that total reserves of Integration Joint Boards (IJB) were lower than the forecast spending gap for 2025-26, and that half of IJBs no longer held any contingency reserves. While the operational gap in 2025-26 decreased slightly compared to the previous year, it still remained at £449 million. Audit Scotland reasoned that IJBs and their partner councils and NHS boards needed to figure out how they would make their services financially sustainable and manage future demand10.
The evidence we have presented suggests that the current way of providing public services is not sustainable, and that people's satisfaction is decreasing. This situation is compounded by a decrease in fertility rates – fewer people are having babies, and there are now more people above the age of 65 than under 16. There is no indication that these trends will reverse.
It would be unfair to say that nothing has been done to improve the provision of public services since the 1944 Edinburgh News article we highlighted earlier in this briefing. The introduction of the NHS for example was called an “outstanding success” in 1998, fifty years after its founding11. But more recently, others have argued that the austerity policies of the 2010s are one of the factors responsible for today's fragility of public service provision12.
There are many suggestions for a revision of the system and many are calling for a shift away from a model where we spend increasing amounts of money on treating problems, towards a system which prevents problems from happening in the first place.
The building blocks of health
We have seen how population changes have put a lot of pressure on public service providers in Scotland, but it would be unjust to blame everything on the ageing population. In this chapter we go a little bit deeper into some of the factors that determine whether an individual will have a good and healthy life, how much reactive, emergency services they will need throughout their life, and when they will need them.
Foundations of health and wellbeing
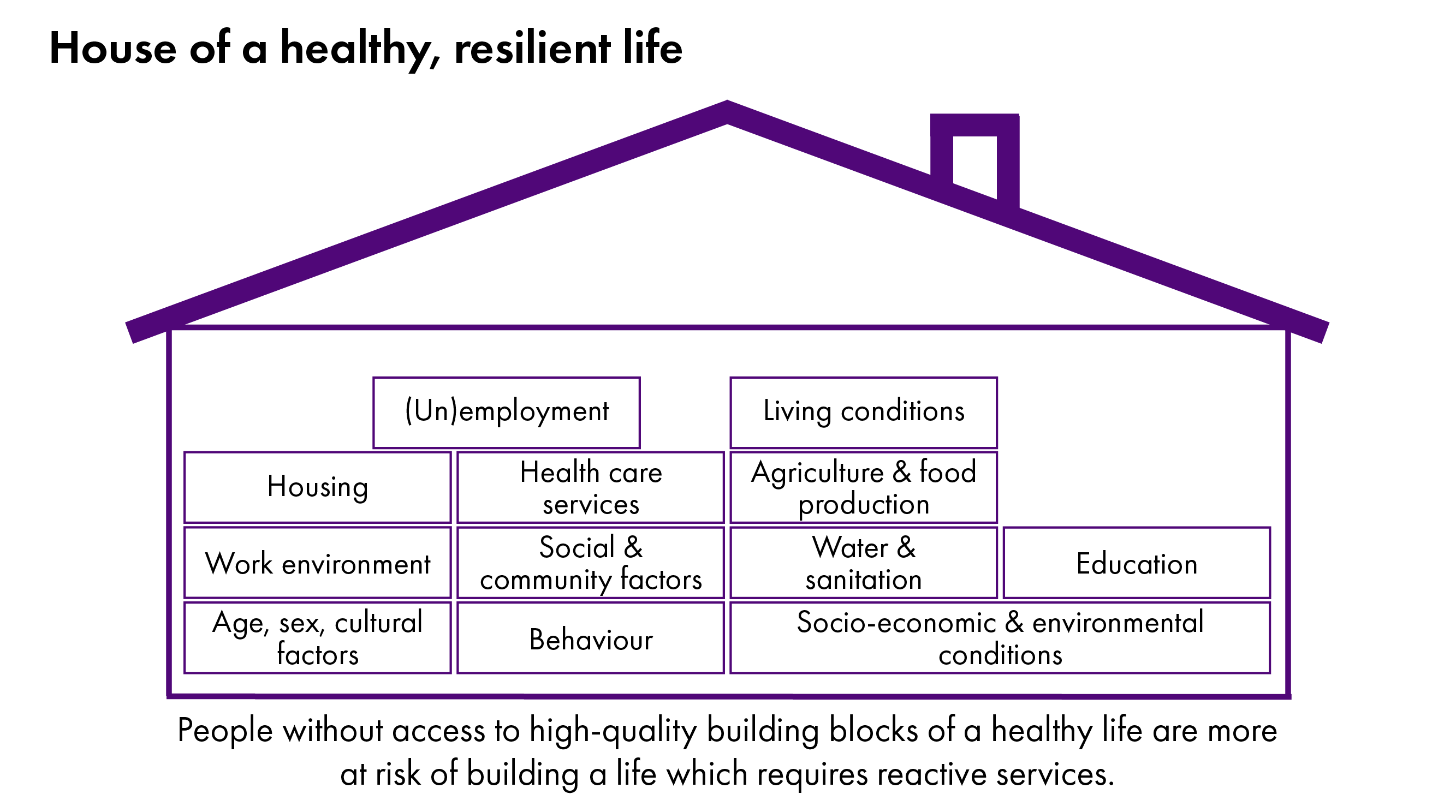
A&E visits and certain social security payments are examples of acute, reactive public services. Both are designed to intervene in an emergency and help someone in a difficult situation get back on track, which makes these services incredibly valuable to society. Arguably, it might be better to avoid a situation where one must seek them out in the first place. The Health Foundation studied which aspects of our lives impact on our health and how long we live for, and published the findings in a report. It pointed out that almost every aspect of our lives influences our health and wellbeing, and it calls these aspects wider determinants of health, or "building blocks of health" (BBH) which is the term we will use in this report.
Public Health Scotland tells us that these BBHs are four times more influential in determining whether a person will be healthy than the work done by health services, claiming that social and economic factors contribute 40%, health behaviours 30%, the physical environment 10% and health services 20%1. We show some examples of BBHs in Figure 6:
The 2024 Health Foundation report What builds good health splits BBHs into several categories to explain what they mean, and how they may influence our health and wellbeing. The below is a shortened version of its descriptions, with much more detail being available in the full report.
Family, friends and communities: Around 1 in 20 adults in the UK report that they always or often feel lonely. Loneliness makes us more likely to experience poor mental and physical health. There are several direct and indirect reasons for this, but an important one is that having positive, supportive relationships can reduce the physiological response to stress, which over time can harm health.
Money and resources: People in the bottom 40% of the income distribution are almost twice as likely to report poor health than those in the top 20%. There is a strong relationship between money – such as income or wealth – and health outcomes. This is because money enables access to many of the other building blocks of health, including good quality housing, healthy food, the ability to heat our homes, and social participation.
Housing: Poor housing affordability is when high rents/mortgages, maintenance costs and utility bills put people under financial pressure. This affects health by causing stress and anxiety, as well as by reducing the funds available to spend on other things that promote health (such as healthy food and exercise). The quality or condition of housing also has a significant impact on health in many ways. Cold homes – or the inability to afford to heat a home – can lead to damp and mould, which can cause respiratory problems, joint pain and headaches.
Education and skills: Education and skills can enable supportive social connections, access to good work, lifelong learning and problem solving, as well as helping people feel empowered. These all enable people to live healthier lives by increasing our ability to live and work in safe and healthy environments, to afford a good quality of life, to access healthy food and activities, and to manage and limit exposure to life's challenges.
Good work: Access to good quality work is a key building block of a healthy society. Good work provides us with sufficient income to meet basic needs, and the money and time to participate in community and social life – all essential to good health. Good work provides stability, security and support for our wellbeing: from hazard-free environments to personal development opportunities, autonomy over our work and a good work–life balance.
Transport: Transport can directly affect health in positive ways, such as the physical and mental health benefits of travelling in active ways, like walking and cycling. Transport can also directly negatively impact on health – air pollution and road accidents, for example. Reliable, affordable and accessible transport also influences health by shaping our access to other building blocks of health, such as connecting us to work, public services and social connections.
Our surroundings: Some aspects of our surroundings have a direct effect on our health – for example, exposure to air pollution increases the risk of asthma and lung cancer. Access to safe green spaces can bring important mental and physical health benefits, offering the opportunity to exercise outdoors and spend time in nature, which is increasingly understood to be good for our mental health. The density of outlets selling tobacco affects the number of young people taking up smoking in a local area.
The food we eat: Everyone should be able to access and afford enough nutritious food to lead a healthy life. Healthier foods tend to be more expensive and less readily available than foods that are high in fat, salt and sugar. The most deprived areas in England have five times more fast-food outlets than the least deprived areas.
The BBHs are not only important in determining health and wellbeing outright, but also in influencing a person's behaviour and leading them to do activities which help their health and wellbeing. BBHs for example influence how likely a person is to take up drinking alcohol, smoking or drugs, but also how likely they are to be physically and socially active. The Health Foundation provides a helpful diagram explaining this graphically. We have reproduced this diagram in Figure 7.
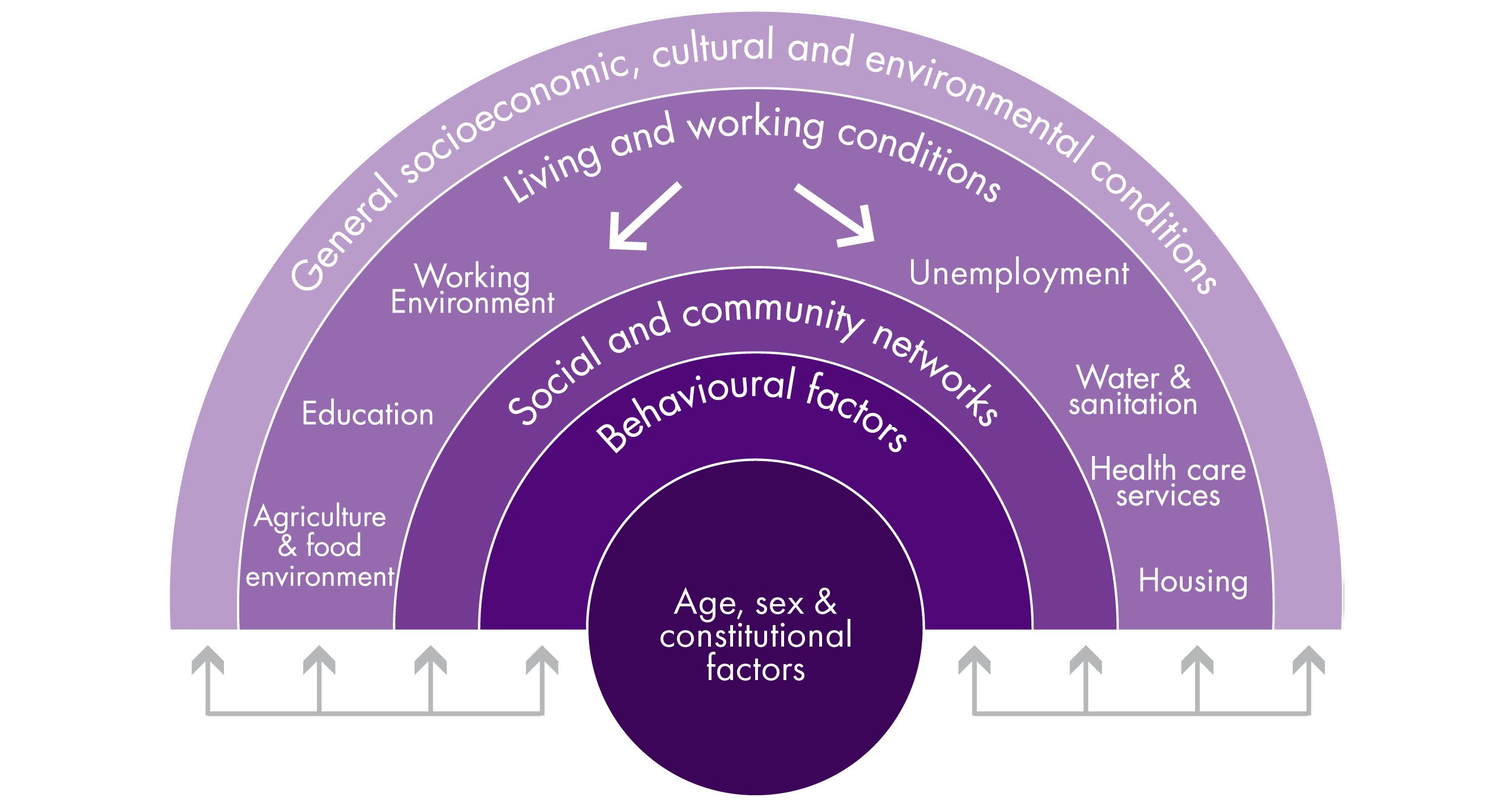
Figure adapted from The Health Foundation's What builds good health report.
Not everyone builds the same house
Many BBHs are linked to wealth, and no conversation about BBHs is complete without addressing how these are connected to socio-economic inequalities. Another report by The Health Foundation, titled Living in poverty was bad for your health long before COVID-19 paints the picture that health and wealth are interconnected:
Income and health can both affect each other – lower income is associated with more ‘stressors’ which can harm health and allow fewer opportunities for good health. Poor health can limit the opportunity for good and stable employment and so affect income.
Tracing the line of thinking across Figure 7 from the outside inwards, it is possible to tell the following story: a person who comes from a wealthy socio-economic background is more likely to have good housing, receive quality education and find a good job. These opportunities make it easier for this person to make friends and build networks, both professional and casual. Factors like having good job, lower exposure to housing anxiety and knowledge about health gives this person resources (time, money, know-how, and ambition) to build healthy habits auch as regular physical exercise, eating well, avoiding addictions, etc.
Combined, this means this person is more likely to build a healthy constitution and less likely to need intervention from public services. They might also need any intervention at a later stage in their life, compared to someone from a less advantaged background. Of course, this model represents a generalisation based on statistics, and individual outcomes will vary based on the personal circumstances of each person, but it does demonstrate likelihoods.
In the Scottish context, some examples of socio-economic inequalities manifesting as inequalities in health and wellbeing outcomes are that:
People living in the poorest areas of Scotland are five times likelier to die from preventable conditions than those living in the wealthiest ones1.
People living in the wealthiest neighbourhoods also get 25 more years of being in good health than those living in the poorest parts of the country1.
People in the bottom 40% of income distribution are almost twice as likely to report being in poor health than those in the top 20%3.
The Scottish Health Survey provides data on indicators such as those shown above. We have selected a few which represent people's access to BBHs and health-determining behaviours, based on the SIMD of the neighbourhood they live in. SIMD is a measure of how deprived an area is compared to other parts of the country in terms of seven domains: income, education, health, access to services, crime and housing.
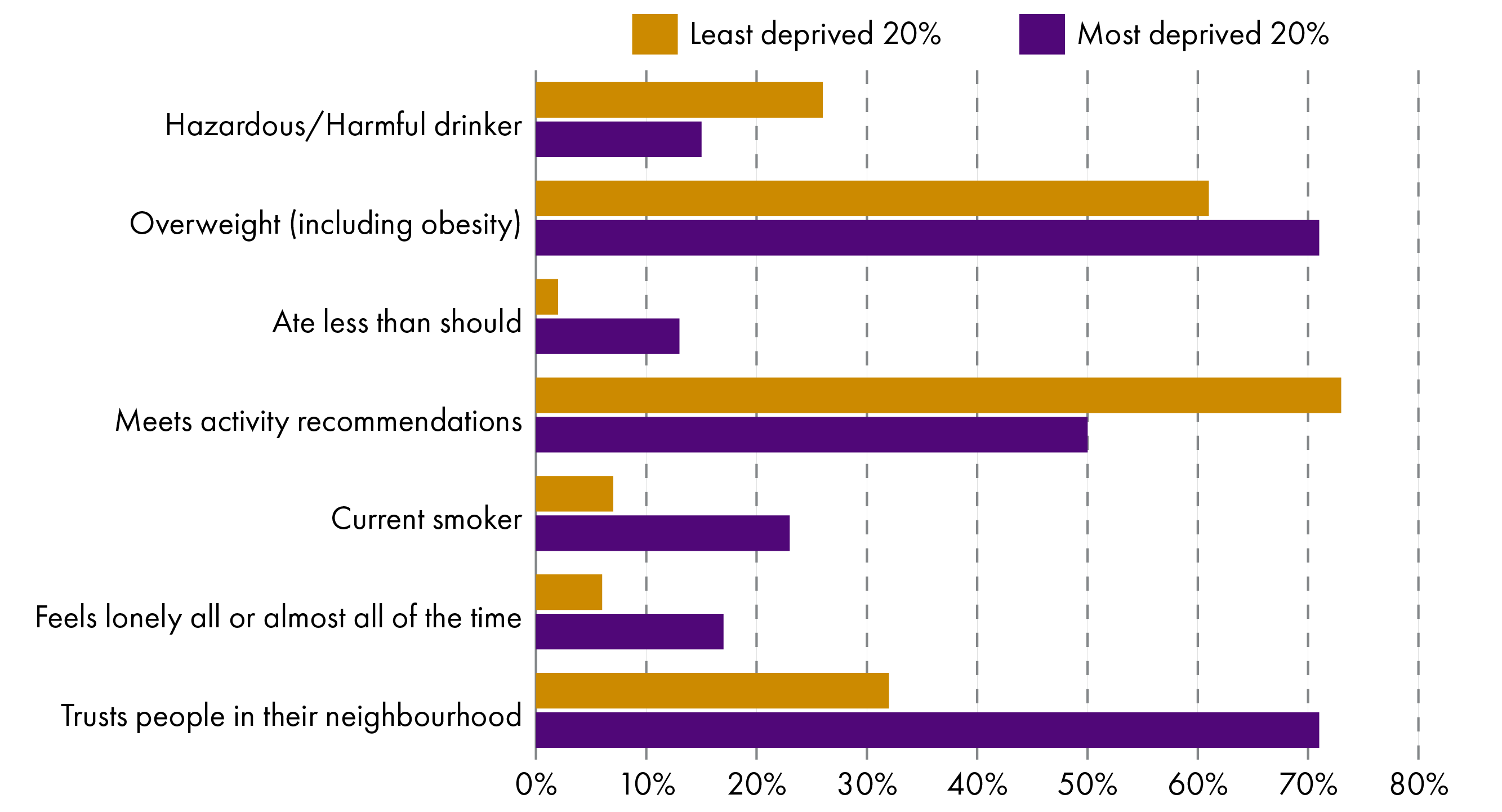
Data from the Scottish Health Survey, indicators broken down by SIMD for year 2022 or 2023 (depending on data availability).
If we then compare this with how people report on their life satisfaction, mental wellbeing, and general health, the link between living a healthy, fulfilling life and living in one of the 20% least deprived neighbourhoods becomes evident. Scottish Health Survey data shows that 79% of people living in the least deprived areas report as being in good/very good health. In the most deprived areas, this is only 56%. People living in the least deprived areas are twice as likely to have above mode life satisfaction. And on the Warwick-Edinburgh Mental Welbeing Scale (WEMWBS), people in the least deprived parts of the country report on average a score of 50, whereas in the most deprived areas, this is 45. Note that the WEMWBS scale is based on a 14-question questionnaire, with scores ranging from 14 to 70. The higher the score, the more positive, cheerful, relaxed and satisfied the person is.
We have seen which are some of the factors that determine if we will be happy, fulfilled and healthy in our life and that these are linked to where we live and our socio-economic background. We have a situation where we know that the current way of providing public services is fiscally unsustainable and failing. We know that people who have access to good building blocks are more likely to build a healthy and happy life. We also know what these building blocks are. Now it is time to think about how public service providers can support people early enough in their lives so that problems can be prevented from arising and more people in Scotland can live a fulfilling, healthy life.
Defining and classifying prevention
In the previous sections we have talked about factors which evidence identified as influential to deciding whether someone will lead a happy, healthy life . If these factors fail, the person might be more likely to seek out reactive, acute care like an emergency appointment or apply for benefits. Preventing such failures and supporting people to be strong and resilient, both physically and mentally, might be a way to drive positive change for people. The old saying goes “Prevention is better than cure”, so in this section we explore definitions of what prevention means with respect to public services.
Most people will have an idea of what prevention might look like: eating healthy food, keeping physically active, seeing a doctor for regular check-ups and so on. However, prevention goes beyond these examples, and even beyond healthcare. There are many definitions of prevention, with two examples provided by PHS and the Scottish Health Equity Research Unit (SHERU).
Public Health Scotland:
Prevention in public health is about keeping people healthy and avoiding the risk of poor health, illness, injury, and early death.
PHS's definition uses the lens of public health to define prevention, which makes it a bit limiting compared to definitions like SHERU's below, which are less health-specific. The Scottish Government uses the PHS definition, but “but adapts it to a broader context that goes beyond health” as described in the Learning from 25 years of preventative interventions in Scotland document.
Scottish Health Equity Research Unit:
By prevention, we are referring to public policy interventions that prevent poor outcomes in the future, as opposed to policy which intervenes to mitigate harms once they have already occurred or subsequently deals with the consequences.
Other definitions are available. For the purpose of this report, we propose the following definition of preventative action (spending, intervention, investment, policy, or otherwise), which is not specific to a particular sector and includes the "primary purpose" principle. The primary purpose principle means only activities designed as preventative count as prevention, not activities which are preventative "accidentally" as a positive externality.
A preventative action aims as a primary goal to reduce an individual's or a population's demand for urgent, reactive public services now and in the future, by removing risk factors, increasing resilience to risk factors, or providing early identification or intervention.
Preventative activity is often split further into categories. In this briefing, we refer to the categories according to the Chartered Institute for Public Finance and Accountancy (CIPFA) definition, as provided in the Understanding Preventative Investment report. The report itself also sets out some alternative definitions provided by Demos and the Scottish Government. Table 2 shows the categories, definitions and examples of what such activity could look like.
| Activity | CIPFA Definition1 | Example |
|---|---|---|
| Primordial prevention | Supports whole populations by changing social, economic and environmental conditions to prevent risk factors from emerging in the first place. | Cars with internal combustion engines emit pollutants, which, when inhaled, can increase the likelihood of respiratory disease. Implementing a Low Emissions Zone (LEZ) changes the environmental conditions and reduces the population's exposure to pollution, thus reducing the risk of respiratory issuesi. |
| Primary prevention | Supports people at risk of problems by reducing exposure to known risks or strengthening protective factors to prevent problems from arising. | Living in cold or damp conditions can worsen asthma and other respiratory disease, increase the risk of heart disease and have a negative impact on mental health. Investing in improved insulation, heating and dehumidifying in exposed communities would reduce these people's exposure to cold and damp and lower the risk of negative impactsi. |
| Secondary prevention | Supports people showing early signs of problems by identifying issues and responding early to prevent them from escalating. | Spirometry tests are a way of checking a patient's respiratory health and are used to identify lung conditions like asthma, pulmonary fibrosis, or lung cancer. Investing in improved spirometry could help patients showing signs of respiratory disease access treatment earlier, improve their health for longer and reduce the number of times they need to see a doctori. |
| Tertiary prevention | Supports people living with ongoing problems by helping them manage their situation and improve stability to reduce reliance on reactive services and prevent problems from further escalating. | For people living with a lung disease, pulmonary rehabilitation is an exercise and education programme, which helps people understand and manage their condition and symptoms. Accessing such courses helps people walk further, feel less tired and breathless and patients report increased activity after having completed the course, leading to an improved quality of lifei. |
| Enabling activity | Activity that is not in itself preventative but is required to support or facilitate the delivery of a preventative activity. | If prevention is to be meaningful and efficient, its impacts must be periodically evaluated via research and surveys. Monitoring the impacts of a new LEZ on the health outcomes of people living close to it is not in itself a preventative activity but is nevertheless required for the LEZ to be as beneficial as possiblev. |
| Reactive/acute service | Activity designed to support basic operations or reactive services but does little or nothing to reduce the likelihood or severity of future demand for reactive activities. | Once a person's situation becomes so severe that they require the use of a reactive service to treat their acute problems, this is no longer prevention. For example, a person living in a location with higher air pollution, in damp and cold conditions, who has not been diagnosed with asthma yet might have to get hospitalised in the winteri. |
In addition to prevention, two more categories are included for completeness: Enabling and Reactive activities. It is good to note that many sources (including the Scottish Government) do not use a separate category for primordial prevention but instead group it together with primary prevention. The logic behind this is that both primordial and primary prevention focus on preventing problems from appearing in the first place by removing risk factors. The difference is that primordial prevention is not targeted, whereas primary prevention targets a group identified as higher risk. In Table 2 we have included primordial prevention as a category for completeness’ sake, but throughout the rest of the report, primordial prevention will also be grouped with primary prevention.
It is important to keep in mind that prevention stretches beyond healthcare. The same principles as explained above using the respiratory disease as an example can be applied to other topics like child poverty or isolation and mental health. Preventative activity seeks to reduce a population's demand for acute, corrective services, which treat symptoms of problems, by improving the Building Blocks of a healthy life and preventing these problems from arising in the first place. It can be thought of as investing in health, rather than spending on treating illness.
Since the BBHs are so wide and improving any of them might lead to a “preventative” investment, even if it is a secondary product of the investment, there is a risk of over-reporting prevention, in other words, saying “everything can be preventative if you look deep enough”. To get around this problem, the OECD System of Health Accounts 2011 defines a boundary for prevention in healthcare as activities which have "the primary purpose of risk avoidance of acquiring diseases or suffering injuries". While this guidance applies specifically to healthcare, the “primary purpose” can be used as a concept across the board. This way we can identify prevention as an activity which purposefully removes risk factors or promotes resilience, as opposed to doing so as a side effect.
CIPFA has developed a brief public access online course which explains in more detail what prevention is.
Prevention as a solution
When it comes to complex problems like reforming public services, there are no silver bullets. Though it might not be a silver bullet, prevention is mentioned as a principle for reform in documents like the Public Service Reform Strategy, the NHS Scotland operational improvement plan, or Scotland's Population Health Framework. With a prevention-based system, more emphasis would be put on long-term thinking, spending, and actions, as an antithesis to the current system, which some claim to be short-termist1.
Prevention came into the spotlight when the 2011 Christie Commission report included it as one of the four principles for public service reform:
Public services are built around people and communities, their needs, aspirations, capacities and skills, and work to build up their autonomy and resilience;
public service organisations work together effectively to achieve outcomes;
public service organisations prioritise prevention, reducing inequalities and promoting equality and
all public services constantly seek to improve performance and reduce costs, and are open, transparent and accountable.
Since then, criticisms of the short-term approach to spending within the public services have become more common and there have been calls for shifting the balance of care and investing in prevention. But what does this mean?
Investing in prevention means devoting resources to support policies and actions which keep people healthy and well, and prevent problems like ill health, poor mental health, poverty, crime, homelessness, or any other problem which a government wants to tackle.
The shift upstream means that rather than treating symptoms, public service providers should be addressing root causes. While this may seem like a logical thing to do, without a strong understanding of the process, the current status, and the objectives, it is also a very abstract goal and certainly not one which is trivial to implement.
Shifting the balance of care is included in the 2025 NHS Scotland operational improvement plan which recognises that acute hospitals are not always the best place for a person to get treated, and sets out how NHS Scotland will support the provision of more care in a community setting, or at home.
The financial narrative behind a shift to prevention is that while there might be higher short-term costs of services due to an increase in preventative spending, in the long-run future demand for acute services will be lower and thus make these services financially sustainable. At the time of writing, there is no evidence in the Scottish context which makes it possible to 1) quantify the cost of increased preventative spending required, or 2) estimate the long-term impact of such spending. Therefore, while this narrative is common and may appear logical, it is difficult to assess in any quantitative sense.
This section will not attempt to make any quantifications or suggestions, rather, it will explain in more detail what this narrative might mean and some of the underlying principles of a shift to prevention. Throughout the evidence presented below, we find some underlying principles of what a prevention-focused delivery of public services could look like and identify some reasons why it has so far been challenging to implement.
Reducing inequalities
Previously we presented evidence which shows how people's health and wellbeing outcomes are primarily determined by their access to the BBHs and exposure to risk factors. We also presented evidence which shows how people living in the more deprived areas have access to different BBHs than those living in less deprived areas and how this coincides with a 25-year healthy life expectancy difference between the populations of the least and most affluent areas. A clear link between health inequalities and prevention is made by the Royal College of Physicians (RCP) in its Bridging the gap guide (2024). The guide specifically says, “Tackling health inequalities is key to improving the health of the country and reducing preventable demand on health services.”
Addressing population health problems via prevention-focused methods means improving people's access to BBHs. RCP says the following on the area of its website focused on health inequalities and prevention:
If we are to prevent ill health in the first place, there needs to be a greater focus on prevention with action on issues such as poor housing, food quality, communities and place, gambling, the availability of tobacco and marketing of alcohol, employment (including how much money you have), racism and discrimination, transport and air quality.
Figure 8 in the section 'Not everyone builds the same house' shows how in Scotland, most of the above issues are worse in the most deprived communities. This creates a link between a system focusing on prevention and a system focusing on the reduction of socio-economic inequalities, and suggests that any systematic change in the approach to prevention and improving people's access to BBHs should be targeted at the areas of Scotland with the lowest SIMD.
Outcome-based resource allocation and accounting
CIPFA's report Integrating care: policy, principles and practices for places suggests a twin track approach where public service providers “ensure that services can deal with existing and immediate pressures, as well as making long-term investments to ensure services are financially sustainable and provide value for public money”. What this suggests is that whatever long-term preventative investments happen, these will need to be done in parallel to the provision of emergency services. This is important because it highlights the need to “rectify the current imbalance between acute and preventative service spending”, while managing the immediate problems at the same time. CIPFA's report also mentions that a focus on outcomes (like population health indicators or any other goal the government sets) can highlight inter-sectoral dependencies and help create a shared vision. CIPFA goes on to say that “Good public financial management requires making evidence-based decisions on the allocation of public funds to outcomes and the ability to track and evaluate progress.”
We can understand CIPFA’s suggestion as a call to jointly use acute and preventative services to improve population health and wellbeing, allocating resources between them based on an evidence base which considers the outcomes of spending these resources. The spending on these outcomes, be it on acute or preventative services, should be tied to a coherent set of shared goals of the health and care sector. This brings up one of the principles required to capture the impact of prevention: outcome-based resource allocation.
A Carnegie UK report titled Budgeting for Wellbeing: International Approaches reinforces the point about outcome-based budgeting being used as a driver of change for public services. The authors argue that despite progress in developing wellbeing policies and frameworks, there is limited change to how governments raise and allocate money.
The report tries to answer the following question:
How can fiscal policy - through revenue raising, spending, and budgetary processes - be reimagined to prioritise and deliver improved wellbeing for people?
Carnegie UK's work identified three themes, when trying to answer that question:
Current fiscal structures are fragmented, leading to duplication or counterproductive efforts. There is a potential to align government activity and spending with whole-of-government priorities.
An approach which prioritises wellbeing requires a focus on prevention and early intervention.
Achieving wellbeing outcomes necessitates new tools and approaches within budget processes, which capture complexity, interdependence and long-term impact.
The report makes connections between long-term preventative approaches and the need for a way to capture real costs of policies, including how these policies increase or reduce demand for acute government services. Building a connection like this could help budget and policy makers to better understand the cost of (in)action when it comes to long-term programmes and spending.
A report by Demos called Revenue, capital, prevention: A new public spending framework for the future encourages the reader to think about prevention as an investment. The report claims that in a similar way that capital investment can bring monetary return on investment by paying dividends or other mechanisms, investing in prevention can create returns by lowering the cost of future care and improving people's lives.
To support this claim, Demos references the work of researchers from the University of York, who looked at estimating the cost of saving lives and improving the quality of life. Researchers converted local authority data on mortality, healthcare, and public health expenditure into estimates of responsiveness of mortality to variations between public health and healthcare spending, i.e. How does mortality change if public health/healthcare spending increases/decreases? They expressed this in £/Quality-adjusted Life Year (QALY). They found that creating an additional QALY using public health spending costs £3,800, while creating an additional QALY using NHS money costs £13,5001. QALY is an academic metric for measuring how an activity either improves or extends a person’s life. It is often used as a measure of value-for-money for public health and healthcare spending. One QALY means one year in good health, a year in 80% health is worth 0.8 QALY and six months in 50% health is worth 0.25 QALY.
On the back of this, Demos claims that:
The point is that patient consistent investment in prevention has been shown to deliver results, however, we lack the architecture to do this systematically.
Demos further claims that the current system “incentivises decision making which undermines the allocative efficiency of public spending” and proposes a new category of departmental spending, which ring-fences funds for prevention: Preventative Departmental Expenditure Limits (PDEL).
Presently, HM Treasury sets a total amount of Department Expenditure Limits across all departments, which is in turn split into Resource Department Expenditure Limits (RDEL) and Capital Department Expenditure Limits (CDEL). These same definitions apply in the block grant funding provided to the Scottish Government. Demos proposes PDEL would sit next to RDEL and CDEL.
According to Demos, PDEL would create the following benefits:
A baseline for prevention: PDEL would enable tracking preventative spending over time, including creating an initial baseline, to see whether a shift in public expenditure is being achieved.
Greater accountability: The Treasury, Parliamentary committees and the public could hold Departments to account for spending on prevention. Departments could in turn hold accountable the agencies and other bodies which they oversee.
Signalling: Creating a separate spending limit for prevention would signal its importance and encourage officials and agencies to develop activities on prevention.
Improving long term decision making: Separate prevention spending should help budget-makers avoid a position where they have to chose between helping people in need now and preventing future problems from arising. It could also protect prevention budgets from divestment as a result of rising costs of acute services.
To implement PDEL into the budgeting process, Demos suggests that the Chancellor should create a Preventative Investment Unit within HM Treasury to clearly apply the classification across Departments and start making use of it in budget-making and spending reviews. This would require fundamental revisions to public accounting approaches and it is not clear how this would feed through into Scottish budget allocations.
The PDEL suggestion might also be a tricky one to implement in Scotland at local government level, where the Scottish Government, through the Verity House Agreement in 2023 committed to a default position of “no ring-fencing or direction of funding” in the partnership between the Scottish Government and the Convention of Scottish Local Authorities (COSLA). The agreement does caveat this position by suggesting that ring-fencing and funding direction can be used if there is a clear joint understanding of a rationale for this to be the case. Ring-fencing was also identified as one of the “more complex issues” in the Local Government Information Unit’s (LGIU) The state of local government finance in Scotland report (2023) in which LGIU explained that 57% of the respondents of their survey supported the removal of ring-fencing and directed spending. How this would relate to the concept of prevention is not clear.
Community and home care
Another common topic in discussion surrounding prevention is community and home care, sometimes referred to as place-based services. A 2015 report by the King’s Fund explains Place-based systems of care as being systems oriented around a defined population group, reflecting the local context. The report suggested that a place-based system should ideally define the population group served, identify the right services required and partners to provide them, and develop a shared vision and a set of goals based on the local requirements of the community. The report proposed this in contrast to the system at the time, which it described as built around a “fortress mentality”, and which it claimed was unlikely to meet public service challenges like caring for people with long-term conditions and managing demand for urgent care services. One of the potential benefits of such a system identified by the King’s Fund is the opportunity to “develop services that are financially and clinically sustainable through greater integration of care and a focus on improving population health and wellbeing”. This notion is aligned with the objectives of a prevention-based system of care.
In 2022, independent think tank New Local published a report sharing its view of what A Community-Powered NHS could look like. The report contrasted what the NHS could look like in a community paradigm, as opposed to either a state or market one. New Local identified the state paradigm as having been used between the mid-1940s to early 1980s, the market approach between the mid-1980s to mid-2010s, and the community paradigm emerging in late 2010s. The differences are shown in Table 3.
| The NHS | State paradigm | Market paradigm | Community paradigm |
|---|---|---|---|
| Key organisational principle | Standardisation | Efficiency | Prevention |
| Key problems seeking to solve | Treating illness | Treating illness more efficiently | Preventing illness, alongside treatment when needed |
| Locus of power | Clinician and Whitehall bureaucrat | Clinician and manager | Clinician and community |
| View of service user | Deficit-led: primarily a passive patient | Transaction-led: a customer with choice determined by provider | Asset-led: a participant in their own health and wellbeing |
| View of communities | Not in the purview of services | A source of treatment alternatives through social prescribing | Equal partners with deep insight into effective service response |
| Implementation method | Top-down, uniform model of provision | Targets, performance management and productivity drives | Devolution, culture change and deep community engagement |
| Organisational relationships | Separate specialist organisations | Competition between organisations | Collaboration and shared community led mission across organisations |
| Funding model | Centrally planned funding model | Activity-based funding model | Place-based funding allocations, joint investment in prevention |
| Accountability | Whitehall | Whitehall, across an increasing number of arms-length bodies | Local accountability in the context of a national outcomes framework |
| Approach to engagement | Not widely pursued | Patient feedback sought through closed surveys | Community participation viewed as essential to service design |
| Attitude to data | Quantitative data informs decision-making at the top | Quantitative data informs performance management within different services | Quantitative data, combined with qualitative community insights, informs prevention shift |
Data reproduced from New Local, A Community-powered NHS (2022)
New Local did not propose a single model or a single paradigm, but it did point out three broad principles that could shape the creation of community-powered services:
Principle 1: Community participation in decision-making.
Principle 2: Mobilising community assets.
Principle 3: Growing a community-focused organisational structure.
A community-based or place-based approach to public services gives communities a different role – changing them from being passive recipients of a service, to playing an active part in deciding what the service is, and how it is delivered. New Local claimsed that enabling a shift to prevention, which can reduce demand over the long-term in a sustainable way, will require moving to the community paradigm. It argued that “prevention is not something that can be done to [individuals and communities], rather it must be achieved with them”.
What is preventing prevention?
We have seen evidence pointing to the need for a focus on prevention, and we have presented evidence which describes what this could look like. Now we will explore some of the factors preventing prevention – this includes practical issues of implementation (like current ways of working with budgets, or organisational structures) as well as clarity on aligned goals. Many of the challenges we mention here are related to prevention being a topic which spans multiple areas – multiple government departments, parliamentary committees, budget allocations, and public service providers at the least.
Inconsistent definitions
Prevention can sound like an abstract term, and although definitions exist (as shown in the Defining and classifying prevention section of this report), people will have their own idea of what prevention is and a common understanding of prevention is not always the case. In its report Understanding Preventative Investment, CIPFA repeatedly mentions that prevention should be quantified using shared definitions. As of March 2026, there is no official definition of prevention published by the Scottish Government, which instead adapts the PHS definition to a broader context. A lack of an official, agreed, common definition can make interdepartmental dialogue clunky.
Emma Congreve, deputy director at the Fraser of Allander Institute (FAI) at the University of Strathclyde, highlights in an article on preventative budgeting the need to be clear about what is being prevented. Going back to Defining and classifying prevention, we have seen how one of the ways to identify prevention includes seeing whether the primary purpose of the given activity is to remove risk or increase resilience, thus preventing a poor outcome. Therefore, based on Ms Congreve's article, if an organisation is to accurately present an activity as preventative, it needs to be very clear about what it is trying to prevent at the same time. According to Ms Congreve, it is relatively clear to define prevention outcomes in the healthcare sector, where people know what is meant by poor health, and what are some of the goals of the sector – reducing incidence of preventable illness, narrowing health inequalities, extending healthy life expectancy. But the question of what is being prevented becomes trickier for organisation working towards multiple objectives.
The article sets out the example of a government priority being the eradication of child poverty, showing how this could be achieved using multiple ways – preventing it from occurring in the first place by increasing wages or lowering housing prices or by providing an acute, reactive service such as social security. This way, social security, normally viewed as a reactive service, can serve as primary prevention if one sets the target as improved education outcomes. If the target is reduced child poverty, social security becomes either reactive, or at best tertiary prevention. Ms Congreve points out that this lack of clarity creates room for subjectivity in assessing what is preventative spending, and that subjectivity does not provide a sound basis for objective analyses of the budget or for a systematic prevention shift.
Once there is consensus on what prevention is and what it is that the government and service providers are trying to prevent, there will still be some technical barriers to overcome.
Availability of data
The most detailed level of budget data currently published in Scotland is set out in the Level 4 Budget tables. The FAI article we refered to previously notes that Level 4 data are too aggregated to allow for meaningful analysis of the data from the point of view of prevention. The article suggests that the reason for this aggregation is that the Scottish Government is rarely the delivery body for its policy and services. Public services are instead delivered by local government, regional NHS boards and IJBs, and at a more granular level, procured through arm's length external organisations, and grant funded private and third sector organisations.
For example, in the Scottish Budget Level 4 allocations, there is a £12.4 billion allocation to the NHS Territorial Boards, with no further information on how this funding is split between acute and preventative services. Additionally, information on how each Local Authority allocates money to public service delivery bodies is not always easy to find, even for independent auditors. This creates a situation where it is very difficult to create an understanding of the current level of preventative spending across the Scottish Budget and to scrutinise whether the Scottish Government is delivering on its agenda of focusing on prevention, as mentioned in the Public Service Reform Strategy and other policy documents.
The problem with data is not just its availability. Some commentators suggest that the method in which data are collected is also challenging, especially when it gets used as a metric for compliance with policy. In the Finance and Public Administration Committee (FPAC) meeting on the 9 September 2025, João Sousa, Deputy Director and Senior Knowledge Exchange Fellow at the FAI told the Committee:
One of the problems with some of the categorisation of [preventative spending] within Government is an example of Goodhart's law— once a measure becomes a target, it ceases to have any meaning. If you try to categorise everything on whether it really is preventative or not, are you just encouraging people to put that forward in the preventative lens rather than the acute issues lens?
Put simply – if the Government sets a minimum requirement for preventative spending and asks organisations to report on their level of spending, will this influence how spending is reported?
Cross-departmental nature of prevention
We previously mentioned that prevention is not a matter for a single governmental department or parliamentary committee – investing in BBHs stretches beyond the boundaries of individual departments. To give an example, a good way to prevent respiratory conditions is to ensure people have homes without mould and moisture1. Quality of housing in Scotland is the responsibility of the Cabinet Secretary for Housing, and the Local Government and Housing Directorate. However, if they invest into actions which remove mould and moisture, thus reducing the risk of respiratory disease, any future savings due to reduced demand will likely be felt not by the Local Government and Housing Directorate, but by the Population Health Directorate or other subsidiary public bodies. Ultimately, the investment will be felt by the population where it matters, but accounting for one department's spending when it benefits the outcomes for a different department is challenging. CIPFA picks up on this difficulty in its Evaluating Preventative Investment report:
Benefits are likely to be accrued to different parties to those meeting the costs. Whole system assessment will be required.
CIPFA concluded that this challenge can be overcome by applying a Cost Benefit Analysis on the whole system of public services to create a holistic view. This could capture the performance of the whole system, rather than that of individual departments. CIPFA points to existing tools like the Green Book, Public Sector Accounting Standards Board guidance, or CIPFA's own Prudential Code as all being relevant to such an analysis.
The Scottish Government seems to be aware of this problem, and accordingly commits to “identify, monitor and increase spend on prevention across all public services”, as expressed in a the Cabinet Secretary for Public Finance and Local Government's response to the Finance and Public Administration's 2025-26 Budget scrutiny (13 February 2025). However, in it's report on Pre-Budget Scrutiny 2026-27, the Health, Social Care and Sport Committee expressed that it was not satisfied with the Scottish Government's progress on addressing the cross-departmental challenge:
The Committee calls on the Scottish Government to set out what actions it is taking or plans to take to ensure budget decisions are made in a way that better reflects the cross-cutting nature of prevention in allocating funding.
The cross-departmental issue goes deeper than accounting for costs and benefits. It makes it challenging to scrutinise Scottish Government's work on prevention, because it is unclear which committee should be leading such scrutiny – is it the Finance and Public Administration Committee, the Health, Social Care and Sport Committee, or the Local Government, Housing and Planning Committee? Or, is it all committees with a mainstreamed approach, or perhaps a new dedicated committee? Similarly, it is not entirely clear which organisation would be responsible for implementing the preventative agenda – the Scottish Government sets out policy and strategy, but who oversees the implementation?
A potential solution from a UK perspective is suggested by Demos in its Revenue, Capital, Prevention which suggests that the Chancellor of the Exchequer creates a preventative investment unit. The unit would then apply the prevention classification across departmental budgets. The equivalent in Scotland might be for this unit to sit within the responsibilities of the Cabinet Secretary for Finance and Local Government.
Allocation of funding
The problem with allocation of funding towards prevention is closely tied to the topics discussed in the sections of this briefing on Outcome-based resource allocation and accounting and Cross-departmental nature of prevention.
Due to prevention being a cross-departmental issue, allocating funding for preventative agendas using the departmental budgeting model is tricky, because governments often set whole-of-government goals. For example, the goal to eradicate child poverty is presented in the Scottish Government's Programme for Government 2025 to 2026, but then work towards these goals is progressed through the different departments of Government bringing a risk of silo working. This includes policymaking, service delivery and funding, and is not limited to Scotland.
Carnegie UK's Budgeting for Wellbeing: International Approaches report says that despite governments trying to address complex problems, “…budget practices such as adversarial and department-driven funding allocation reinforces siloing, undermining the ability of governments to take a strategic and coordinated approach to making progress on whole-of-government priorities.” This shows how the cross-departmental nature of prevention directly poses a challenge to budgeting towards preventative activities, because these activities do not fit neatly within the structure of government departments around which budgets are formed. The Carnegie UK report says:
Budget and fiscal processes that concentrate on fiscal targets and budget allocations prior to consideration of goals or missions, necessarily limit the ambition and resources of governments in pursuing whole-of-government wellbeing goals. This makes it much more likely that governments will fall back into old patterns, assigning inadequate (however big they seem at the time) and time-limited funds, into an existing siloed and short-term system, to tackle difficult problems that have repeatedly resisted previous efforts.
The 2012 report by the World Health Organization (WHO) titled Inter-sectoral governance for Health in All Policies: structures, actions and experiences warns that “Health promotion is unlikely to feature prominently as a key goal for most government departments and non-health sector budget holders.” And that “…the predominance of vertical policy structures and funding silos means that, unchallenged, many health concerns that potentially could be addressed through actions outside the healthcare system remain of low concern to these policymakers.” To address this, WHO suggested “Creating a dedicated budget for a non-health sector health-promoting activity, bringing together resources from the health sector and beyond…”. The report sets out other approaches to joint budgeting using which departments can work together to address issues which span more than just one sector.
Another factor which makes finding money for prevention tricky is one of the things it is trying to solve – the financial emergency within public service delivery bodies, which has led to prevention spending being cut to provide short-term funding for front-line services.
In an open letter to the Chancellor of the Exchequer in October 2024, officials from The Health Foundation, Demos, Institute for Government and CIPFA pointed out that, between 2009 and 2023, local authority spending on long-term services in England was cut by three quarters, while spending on looked-after children and safeguarding rose by more than half. The authors of the letter warned that, given the current pressure on public finances, there is a risk that prevention spending will be further squeezed to meet short-term needs, thus undermining the UK Government's commitment to taking a long-term prevention-led approach to public services. They also highlighted that the fiscal frameworks in place did not distinguish between acute and preventative spending.
Benefits can be hard to measure
The subject of “value for money” is often brought up in debate about the financing of public services. While there are some studies which try to estimate the cost of quality-of-life improvement through public health services1 and compare the value to acute healthcare, this has so far been under-explored in the Scottish context. There is no study which would create a comprehensive matrix of how improving each BBH influences health outcomes and wellbeing for the recipients of the benefit. On the other hand, the costs of acute treatment for NHS patients are well known. Therefore, there is a situation in which preventative spending might seem speculative, while with acute “front-line” spending, estimating how much is required to help an individual can be done reasonably accurately. This might incentivise some budget-makers to prioritise spending with a known outcome over long-term, more speculative spending.
Some evidence even suggests that the benefits of using prevention to reduce the incidence of certain diseases could be felt in Gross Domestic Product (GDP) growth values. A 2024 paper by researchers at the Tony Blair Institute for Global Change built the case for prevention by highlighting the potential macroeconomic effects of improving population health. The researchers estimated that a 20% reduction in the incidence of six major diseases keeping people out of work could raise UK GDP by 0.74% within five years, which would be equal to an annual boost of £19.8 billion. They also mentioned that there could be additional savings due to increased tax revenues and reduced benefits payments.
This shows that estimating the money-related effects of increased population health due to prevention spending could really be a complex process, considering not only the costs and benefits to the public service system itself, but also wider direct, indirect, and induced benefits to the economy. The Green Book, HM Treasury's guidance on appraisal, reminds us that “The scope of all appraisals is UK society”, which, depending on interpretation, could suggest that an appraisal of preventative policies and spending should include a whole-of-society scope.
To add another layer of complication, not all of the benefits of prevention can be measured in monetary terms – sometimes the benefit is someone living longer, or having a better quality of life, and this may not have financial implications for the individual, or for the Government.
The National Institute for Health and Care Excellence considers treatments which cost below £20,000 to £30,000 per QALY to be cost-effective2. While some consider QALY to be the academic standard for measuring cost-effectiveness3, others point out that it is not clear how or if the costs and benefits which fall outside the scope of NHS services are included in the QALY model4. Some academics have even said that “The Math Doesn't Work” when referring to how QALY can measure cost-effectiveness of health interventions5. HM Treasury provides further discussion of how to quantify wellbeing in its Wellbeing discussion paper: monetisation of life satisfaction effect sizes, published as supplementary guidance to The Green Book.
Change takes time
Throughout this briefing, we have highlighted how prevention can be described as 'trying to prevent future problems from happening' and that it is, in many cases, a long-term investment. It follows that seeing the benefits brought forward by preventative spending might take some time. The Local Government Association tried to demonstrate the social return on preventative spending in its report, Earlier action and support: The case for prevention in adult social care and beyond. The report presents a table of maximum time over which the authors expect to see the benefits of investment in select preventative interventions in adult social care:
| Intervention | Maximum time over which the estimated benefits would be realised |
|---|---|
| Supporting people (housing-related services) | 2 years |
| Going the Extra Mile (Employability support) | 5 years |
| Partnerships for Older People Projects (Reducing social isolation or exclusion among older people) | Over 5 years |
| Community Champions (training local volunteers) | 5 years |
| Local Area Coordination | 10 years |
| Small but Significant (handyperson services) | 5 years |
| Falls Prevention Programmes (home assessment and modification) | 2 years |
| Community-Led Support | 1 year |
| Estimated average | 3.02 years |
Data reproduced from Local Government Association's Earlier action and support: The case for prevention in adult social care and beyond report.
The time for benefits to realise varies based on the intervention, but in nearly all cases it is longer than the time-frame for budgeting activities. Given that both UK and Scottish Budgets cover a period of one year (with occasional Spending Reviews covering a 3-5 year time-frame at most), understanding and acting on the impact of spending interventions within budgetary windows would be challenging.
Summary of challenges
There is a strong case for a shift to prevention as a guiding principle for public services, and while the Scottish Government recognises this, carrying out this shift is no small task. There is a lack of data underpinning the current level of spending on prevention, and collecting this data is difficult. Estimates on the benefits of prevention are also problematic, because the effects may be complex in terms of their cross-departmental nature, economic effects, non-monetary value, and a time delay in realisation. The shift to prevention itself is made systematically difficult by the vertical structure of government work organisation and budget creation. Finally, it is becoming increasingly difficult to find money to invest in preventative interventions, because of the very reason behind the proposed shift to prevention – unprecedented demand for reactive public services, which costs more money than ever, so that less is available for long-term projects.
Despite this challenging situation, the Scottish Government and committees of the Scottish Parliament are trying to make progress with prevention. In the next section we look at their work, and at how prevention is finding its way into scrutiny, policy, and legislation, as well as exploring some examples from abroad.
Prevention in policy and government
We have presented evidence for why some think a shift towards prevention is a way to help the sustainability of public services, looked at ways in which prevention is defined, and some of the principles for its implementation in practice. We have also explained why this implementation is not trivial. In this section, we talk about how the Scottish Government, Scottish Parliament and other organisations have included prevention as a principle for their work.
A lot of the evidence discussed in this section emerged as a response to the situation described in the first section of this briefing, and as a result includes the Scottish Government's own definitions of the situation, and of prevention.
Public Service Reform Strategy
"Ensuring high quality and sustainable public services" is one of the four priorities described in the Scottish Government's Programme for Government 2025 to 2026. The programme identified that “Much of the pressure in our health system stems from conditions which are preventable earlier in life – but which are also often symptoms of inequality.” The Public Service Reform (PSR) Strategy, published in June 2025, presents the Scottish Government's plan to improve outcomes, reduce inequalities and ensure fiscal sustainability, quoting a “strong focus on efficiency and a prevention-first approach”. The visions and beliefs set out in the Strategy are presented as follows:
Public services are critical to delivering a fairer future and the Government's priorities of eradicating child poverty, growing the economy and tackling the climate crisis.
Public services are both an asset and an investment in our health, equality and prosperity. That investment should be efficient, effective and targeted where it makes the most difference.
Public services need to be protected for the future by using investment wisely, optimising the value of every pound.
Public services should be accessible, trusted, good quality and meet the needs of people across Scotland.
Complex issues can rarely be addressed in silos and often require integrated solutions informed by deep local knowledge.
These goals resonate with much of the evidence we have presented in this briefing (see the section which describes Prevention as a solution), and indeed the PSR Strategy specifically mentions the findings of the Christie Commission on the future delivery of public services. In his foreword to the Strategy, Minister for Public Finance Ivan McKee acknowledged that the vision of the Christie Commission had not been delivered to its full potential, and explained that the PSR strategy aims to address this challenge. The foreword referenced the First Minister's words when speaking to the Budget for 2025-26 at a University of Edinburgh event, in which he spoke of the twin commitment of “Delivery in the present, hope for the future”. This echoed the principles and “twin track approach” identified by CIPFA in its 2022 report, Integrating care: policy, principles and practices for places. The Government explain that the PSR strategy builds on principles developed in response to the Christie Commission's findings (which are also used as a basis for the Health and Social Care Service Renewal Framework).
| Prevention | Place | Partnership | People | Performance |
|---|---|---|---|---|
| Prioritising spend on public services which prevent negative outcomes and further demand for public services. | Integrated services at local level that are locally responsive and focussed on improving lives. | Public service providers working in partnership, integrating service provision to improve outcomes. | Empowerment of individuals and communities through involvement in the design and delivery of services. | Delivering maximum value for every pound of public money spent, and being able to assure the public that this is the case. |
Adapted from the Scotland's Public Service Reform Strategy: Delivering for Scotland report.
The PSR Strategy is formed by three pillars: Prevention, Joined up services, and Efficient services. Each pillar is then split into work-streams.
| Pillar 1: Prevention | Pillar 2: Joined Up Services | Pillar 3: Efficient Services |
|---|---|---|
|
|
|
In the PSR Strategy, the Scottish Government also proposes methods for measuring and monitoring progress. Each workstream has its own governance and evaluation methodology. At an overarching level, the Scottish Government proposes that the Public Service Reform Board will bring together input from public bodies, local government, and the third and private sectors to advise and scrutinise the Government's progress on PSR work. The Government wants to drive change using a portfolio management approach, and to support evaluation it is working on a Theory of Change and Monitoring, Evaluation and Learning Framework. The PSR Strategy is also subject to statutory duties on reporting impact assessment, with the Government publishing these assessments in a combined document shortly after the announcement of the Strategy.
The Strategy document points to previous examples of reforming public services in Scotland, and the Scottish Government's indicators of success for these reforms. These include reform of youth justice services in 2008 leading to a 92% reduction in the number of 12-17 year-olds proceeded against or receiving custodial sentences, the Police and Fire Reform (Scotland) Act 2012 leading to reform savings in the police and fire service, and improved outcomes through the Scottish Child Payment and the Cashback for Communities programme.
Evaluation and Parliamentary scrutiny
The Parliament's Finance and Public Administration Committee monitors the Scottish Government's progress on delivering the Public Service Reform Strategy. In the report on FPAC's pre-Budget scrutiny 2026-27 (October 2025), the Committee asked the Scottish Government for further information on the Change and Monitoring, Evaluation and Learning Framework relating to the PSR Strategy. In its response to the Committee on 13 January 2026, the Government reiterated that the Strategy commits to a Change and Monitoring, Evaluation and Learning Framework, where “Each work-stream will have its own monitoring and a system wide evaluation will also be undertaken to ensure coordination” and gave an indicative timeline of“early 2026”. At the time of writing, the Framework had yet to be published.
The latest official Scottish Government update on PSR progress from 18 July 2025 mentioned several updates along Pillar 1: Prevention of the PSR. These included the publication of the NHS Operational Improvement Plan, the Health and Social Care Service Renewal Framework, Scotland's Population Health Framework.
Aside from plans and frameworks, the Scottish Government's update presented some evidence of action by mentioning The Food (Promotion and Placement) (Scotland) Regulations 2025. These regulations specified new rules around where less healthy food could be placed in retail outlets, restrictions on how specific foods could be promoted online, and restrictions on volume and price promotions for certain foods and drinks. As an example, the legislation specifies that certain foods, like soft drinks or confectionery, cannot be placed within 2 metres of a checkout facility or queuing area unless it is on shelving at the end of an aisle (with exceptions for smaller premises).
Population health framework
The Scottish Government and the COSLA set out their long-term approach to improving Scottish public health and reducing health inequalities in the Population Health Framework (PHF) in June 2025. In a joint foreword, the First Minister John Swinney and the president of COSLA Shona Morrison acknowledged that “…as much as 80% of what affects health happens outside the health and care system”, and went on to present a vision of improving health and wellbeing and preventing poor health by tackling root causes of ill-health. The PHF has two aims:
Improve the life expectancy in Scotland.
Reduce the life expectancy gap between the 20% most deprived local areas and the national average by 2035.
The PHF structure is influenced by the four health pillars presented in The King's Fund's A vision for population health: towards a healthier future (2018) and the “Marmot principles” identified by the Professor Sir Michael Marmot in the Fair Society, Healthy Lives (The Marmot Review) report in 2010. The drivers of wellbeing which form the structure for the framework are shown in Figure 9.
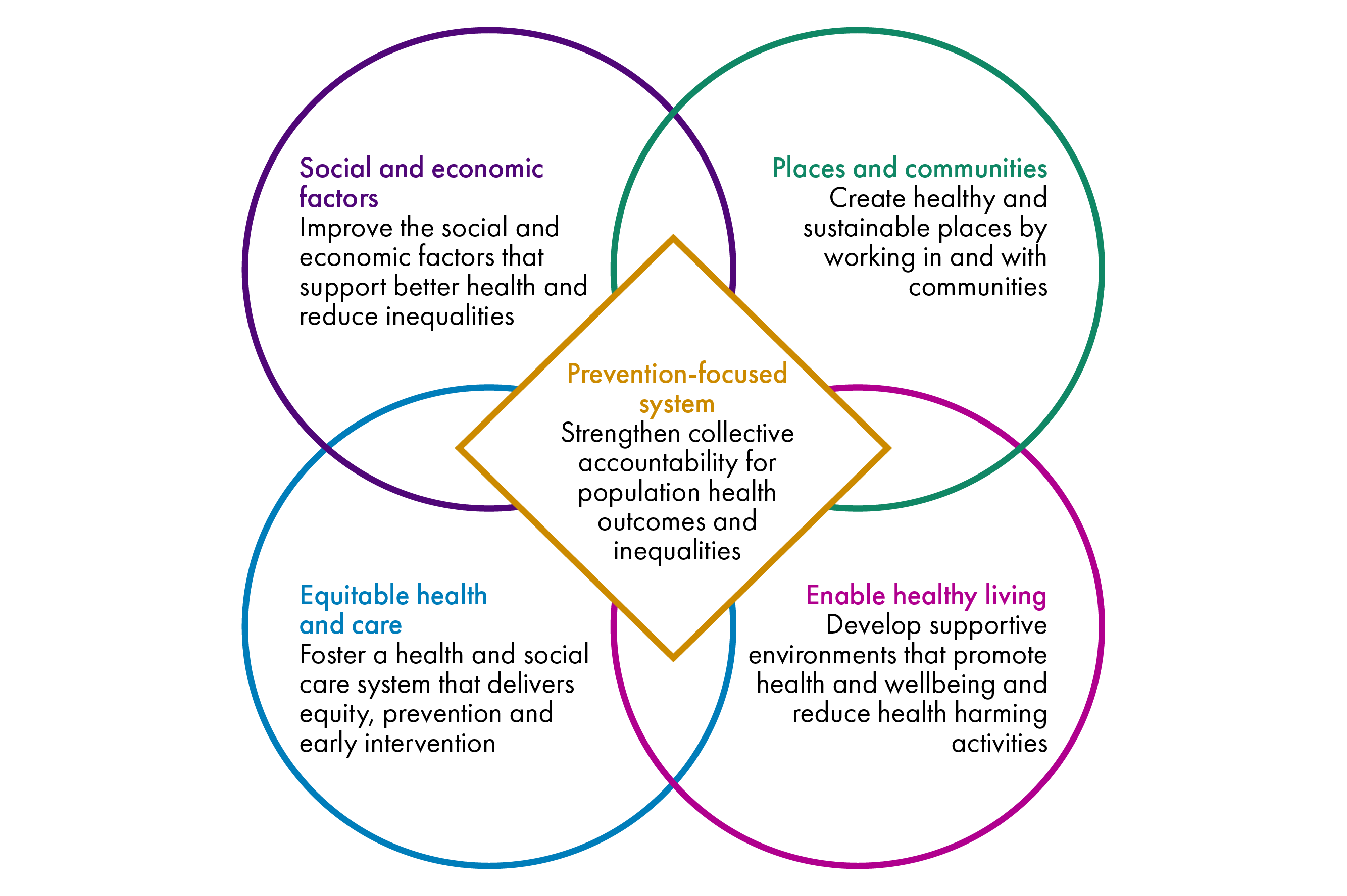
Created using data from Scotland's Population Health Framework.
In addition to this structure, there are four guiding principles to the Population Health Framework:
Prioritise creating and maintaining good health and preventing ill health.
Change systems and environments to support individuals to stay healthy.
Focus support on the people and communities who need it the most.
Deliver through a whole system approach – nationally and locally.
The PHF presents a long-term plan to improve the two outcomes we have stated at the start of this section by 2035, but there are partial milestones as well. The Scottish Government identifies two initial priorities for delivery between 2025-27:
Embedding Prevention in our Systems: Develop mechanisms that prioritise addressing inequalities and improving prevention within planning, delivery, budgets and accountability.
Improving Healthy Weight: Develop a whole system approach to improve food environments; ensure a healthy, balanced diet is accessible and affordable to all; and improve population levels of healthy weight.
Public Health Scotland published a blog welcoming the PHF, noting that it marks a shift in the approach to health, and that the strategy makes it clear that responsibility for health extends beyond health care providers. PHS's new 10-year strategy is aligned with both the PHF, and with the Service Renewal Framework. In addition, at the point of publishing this briefing, PHS listed the PHF among other interventions on its web page on Action to improve public health in Scotland.
National performance framework
The National Performance Framework (NPF) sets out a vision of wellbeing for Scotland. As of 5 March 2026, the NPF is under review, SPICe published a blog talking about the changes. The draft of the updated version was sent to Scottish Parliament committees, including FPAC (which leads scrutiny on the Framework) on 16 February 2026. The (draft) NPF presents Scotland's National Outcomes, which represent the Scottish localisation of the UN Sustainability Development Goals. The Scottish Government introduces the NPF as follows:
The proposed National Performance Framework (NPF) has been designed as a compelling and aspirational vision of sustainable and long-term wellbeing for the people of Scotland. It encompasses our social, economic and environmental needs, and is intended to provide a clear vision for a future in which we all want to live.
The proposed NPF takes inspiration from international examples of strategies which consider long-term effects of policy on wellbeing: the Welsh Wellbeing of Future Generations, New Zealand's Living Standards Framework, Austria's How's Austria? and the German Wellbeing in Germany. These initiatives try to report on wellbeing indicators in the country and some make sure that future wellbeing is considered in lawmaking.
The Community Empowerment (Scotland) Act 2015 requires the setting of national outcomes – specific, high-level goals which the Scottish Government is working towards. The Scottish Government in its proposals for the revised NPF explains that it has developed six national outcomes for Scotland, and says that these are not to be viewed in isolation or thought of as any one person or organisation's responsibility. As a cross-cutting theme, the national outcomes must “have regard to the reduction of inequalities of outcome resulting from socio-economic disadvantage”. The outcomes aim to present a Scotland which is:
Connected – We participate freely in the civic, cultural and social life of our communities. Healthy – We live longer, healthier and more fulfilling lives.
Prosperous – We have a successful economy which supports a good standard of living for everyone, with fair work and the opportunity to thrive.
Secure – We live safe lives, free from violence and injustice.
Skilled – We have the knowledge and skills we need throughout our lives to realise our full potential.
Sustainable – We live in a healthy environment, enjoy the natural environment and protect it for future generations.
To measure progress of these six outcomes, the Scottish Government is developing a set of indicators, which it aims to fit the following criteria: “relevance, coherence, balance, technical quality and international alignment”. Work on this will be reviewed by the Chief Statistician, and the NPF Technical Advisory Group. It will then be for the new Parliament formed after the 2026 Scottish election to consider these proposals.
The Scottish Government outlines what it thinks work towards the NPF goals should look like: long-term and strategic, collaborative, and inclusive. The first point is very relevant to prevention. The Scottish Government explains that it wants to build the NPF in such a way that it will help decision making and budgeting to focus on and be accountable for “improving people's lives and public services now and in the future”. While this is in line with the aims of a preventative system, at the point of publishing this briefing there is little detail on how the Scottish Government plans to achieve this. However, based on the NPF proposal, it appears that the Scottish Government intends to publish “ways of working” for the NPF, and these might include some provision for preventative approaches, as is the case with the Welsh Wellbeing for Future Generations or with the Christie Commission principles.
As of March 2026, the Scottish Government is engaging with various stakeholders to formulate the new NPF. The future timeline is indicated by the Government as follows:
We would expect a Scottish Government motion for debate to be made following summer recess, subject to parliamentary business. We would also propose that implementation plans or statements of intent are published on respective websites by end-2026.
Scottish Parliament's committees and prevention
The committees of the Scottish Parliament are closely following the Scottish Government's work on prevention from various points of view. In this section, we look at how prevention has come up in budget scrutiny and in talks about the Climate Change Plan, among other things.
Budget scrutiny
In its role as lead committee on budget scrutiny, the Finance and Public Administration Committee scrutinises whether the Scottish Government is forming budgets which consider the strategies it has set (like the PSR Strategy), and whether it is doing this with fiscal sustainability of public services in mind. In FPAC's Report on pre-Budget scrutiny 2025-26, the Committee noted that it was “encouraged by the focus on preventative and early intervention approaches within the Scottish Government's PSR programme” and asked the Government to report to the Committee on benefits, risks and costs or introducing a new category of public expenditure on preventative spending. To this, the Cabinet Secretary for Finance and Local Government responded that the:
Scottish Government is taking forward work on preventative spend as part of the PSR programme and will update the Committee in due course. This work will include developing case studies examining post devolution examples of prevention that have resulted in improved outcomes, cost savings and / or reduced demand.
A similar exchange followed during FPAC's 2025-26 Budget scrutiny when the Committee welcomed the “renewed focus on prevention” contained in the PSR, but pointed out that it was “unclear from the Scottish Government's response to [FPAC's] pre-budget report whether it has accepted our recommendation that it considers and reports back to the committee on the potential benefits, risks, and costs of introducing a new category of public expenditure on preventative spend”.
The Government's response to the Convener from 13 February 2025 noted that while “classifications of public expenditure as set out in the Budget document are dictated by the UK public expenditure framework within which the Scottish Government is required to operate”, it is committed to exploring how spending on prevention can be identified, monitored and increased and that analytical work is being done on this topic to underpin the PSR. The latest PSR update, from 18 July 2025, informed the Committee of the publication of the PSR strategy, but did not provide a concrete answer to the Committee's question about the methodology, or any results of the identification, monitoring or increase in prevention spending.
FPAC requested more information from the Scottish Government on progress towards tracking and measuring the outcomes of preventative spend in its Report on the Scottish Budget 2026-27. In her response, the Cabinet Secretary for Finance and Local Government highlighted the Government's pilot activity on budget tagging:
The preventative spend budget tagging approach is currently being developed as part of a pilot process across Scottish Government portfolios and wider public sector partners. The pilot process is expected to conclude in Q2 2026, after which a methodology will be agreed with partners that can be used as part of a wider approach across the full Scottish Budget.
The Local Government, Housing and Planning Committee has also expressed concern about the “slow pace of change since Christie”. For instance, during its pre-budget scrutiny 2025-26 the Committee expressed frustration with the paradox of there being a wide acceptance of the need for a shift to prevention within local government services, but “limited evidence of such a shift actually happening in practice”. In her response to the Committee, the Cabinet Secretary informed the Committee that as part of the PSR programme, the Scottish Government was taking forward work on preventative spend, which includes developing case studies of prevention improving outcomes, reducing demand or providing cost savings. The Cabinet Secretary also mentioned joint work with COSLA on the Local Governance Review:
Proposals for a move towards single authority models in three authority areas reflect the potential of place-based approaches to enable systems reform. Alternative local governance arrangements would enhance local leaders’ ability to shape service provision in light of local circumstances and deploy budgets in ways which support a vital shift towards prevention.
The Health, Social Care and Sport Committee made a series of recommendations around prevention in its 2026-27 pre-Budget scrutiny. Specifically, the Committee asked the Scottish Government to regularly publish data on preventative spending. At the same time, it asked the Government to lay out its plans for ensuring budget decisions are “made in a way that better reflects the cross-cutting nature of prevention in allocating funding.” This is an important request, due to reasons which we have outlined in a previous section of this briefing.
The Cabinet Secretary for Health and Social Care, in his response to the Committee, gave more detail on the Prevention Project, being the budget tagging pilot that the Government is carrying out to identify the current level of preventative spend across the budget (which we cover in more detail on our section on the Scottish Government's work on prevention). He explained that the outcomes of the pilot will inform further action about publishing guidance for budgeting, definitions, and a comparison of how preventative spending shows up across budget lines.
Climate Change Plan
The Health Committee also considered prevention within its scrutiny of the Scotland's (Draft) Climate Change Plan (CCP). The CCP sets out policies which will allow Scotland to meet carbon emission reduction targets, and how this will be done fairly, as a “Just Transition”. The draft CCP states that:
The CCP will support delivery of Scotland's prevention-focused Population Health Framework, wider public service reform agenda and the ambitions of the Scottish Government to build a fairer, greener and healthier Scotland.
The CCP further states that the proposed policy actions can protect people and communities from risks associated with fossil fuels and provide health benefits from cleaner air, healthier food, warmer homes and more. The Committee considered and scrutinised the draft CCP in a series of meetings at the start of 2026. During evidence-taking, Professor Jill Belch noted that air pollution contributes to health inequality and that reducing it would create benefits, and in this regard, there might be a positive effect of the policies within the draft CCP on population health. Professor Sir Gregor Smith talked about prevention more specifically. He mentioned that a preventative approach to health, which reduces demand for treatment of preventable problems could help human as well as planetary health by reducing the environmental impact of care provision.
When asked what the Parliament should be doing to support the preventative agenda politically, Professor Smith responded by encouraging the Parliament to emphasise prevention work when creating metrics of performance:
In the metrics and measurements that we use to assess how our ecosystem is performing, I would like much greater emphasis on some of the prevention work. That is really important. Tracking exactly where our spend is through some of the proposed mechanisms, such as budget tagging and so forth, is another important aspect.
It is also about the degree of scrutiny that we have all placed on the NHS in its role as a body to fix ill health. We need to flip that to challenge and scrutinise the NHS and the other organisations that are involved, such as local government, on their contribution to the prevention agenda. Ensuring that we have the right measurement framework to do that is one of the most important things that this committee can contribute to in future.
Summary of committee scrutiny
In this section we have shown how various committees have considered prevention and preventative approaches, and that this often links to overarching strategic approaches such as Public Service Reform and the National Performance Framework, and to Budget scrutiny. Much of the communication between committees and the Scottish Government shows a back and forth on commitments and strategies for prevention. However, as Session 6 of the Scottish Parliament draws to a close, committees had yet to receive a direct response on how exactly the Government intends to monitor and evaluate progress on the prevention agenda. Such detail is essential for committees to be able to effectively scrutinise progress against the prevention agenda and it will now be for Session 7 committees to consider how they will progress this.
There are hints that more clarity will come when the Scottish Government publishes the results of the Prevention Project pilots later on in 2026. Though committees have heard evidence about prevention being an all-Government all-sector topic, there has to date been no cross-committee scrutiny of the Government's preventative agenda.
Scottish Government and prevention
The Scottish Government recognises the need to progress the work on prevention and is currently working to create an understanding of the current state of play. As we noted in the previous section, the Scottish Government provided an update on progress around preventative spend to the Health, Social Care and Sport Committee on 24 February 2026. This is an important step: stakeholders want to know what is being done now, what the situation is and they need guidance for how to get involved. The progress update mentions that the Scottish Government aims to tag preventative spend across the Scottish Budget and create an understanding of the status of spending on prevention across departments using a pilot project. The Scottish Government has worked with stakeholders to develop common definitions of prevention, building on work by PHS, CIPFA and OECD. The Scottish Government says the pilot project is delivering on workstreams 5 (Understanding and mitigating demand drivers) and 6 (Preventative budgeting) of the PSR agenda. In its NHS Scotland 2025: Finance and Performance report, Audit Scotland welcomed the Scottish Government's publication of the Operational Improvement Plan, Health and Social Care Service Renewal Framework, and the Population Health Framework. However, in the same paragraph, it warned of a “persistent implementation gap, between policy ambitions and delivery on the ground”.
We spoke to a source within the Scottish Government to get further details about the work it is doing on prevention. Our source said that one of the outputs of the Scottish Government's pilot will be a tool which will enable the tagging of spending that contributes to improved quality of life. This tool categorises spending as primary, secondary, and tertiary prevention, spending which enables prevention and spending on acute services. Such tagging often requires more detailed data than the Level 4 information published alongside the Scottish Budget. The Scottish Government said that the Government is asking public service delivery bodies for cost-centre level data to improve accuracy of the tagging exercise. To make it as easy as possible and not add too much work to the audited organisations, the target is to use data which can be collated and supplied through roughly two days of work. Although this limits the level of detail which can be provided, it also improves the chances of collecting data from more organisations without negatively impacting on their workload. The Scottish Government also mentioned that a common classification issue is that people classify too many activities as preventative. To get around this, the “primary purpose” principle is applied, where an activity is only classed as preventative if its primary purpose is an improvement of the quality of life (targeting health outcomes, poverty, crime…).
The Scottish Government is piloting the tool with regional NHS boards and local authorities; this should be finished by April 2026. The findings and the tool itself will then be made available for public service delivery bodies to use, starting with a retrospective tagging of the Scottish Budget 2025-26 . This first whole-budget use of the tool will provide a baseline of how much is being allocated to prevention now (or rather was allocated in 2025-26), the report on this is expected later in 2026. Beyond this, we heard that the Scottish Government plans to use the tool to assess the 2026-27 budget and include it in the creation of the 2027-28 budget to make sure more spending is going to prevention, in line with the PSR strategy. This may require some additional work to make the tool possible to use in budget creation, rather than in retrospective budget tagging. Either way, it should make it possible to create a time series of preventative spending over at least three budgets to see some initial trends.
The Scottish Government also intends to publish portfolio-level breakdowns of preventative spend, allowing committees to scrutinise the development over time and the degree to which the Government is keeping to the target of shifting investment upstream. Over time, it should be possible to scrutinise whether preventative investment and the PSR are delivering long-term positive impacts on the sustainability of public services, and on people's lives in Scotland. There are also parallel trials of outcome-based budget tagging, which, if successful and in combination with the “pilot” of outcome-based budgeting using the point of view of prevention, could create a better understanding of how to target investment to contribute to Government goals.
A lot seems to be riding on the result of the Scottish Government's Prevention Project. It has the potential to shape the future progress of this area of policy by providing a precedent for how things are done. It should provide tools to measure and evaluate progress and might influence future policy-making and budgeting activities. It will be very interesting to see the results, which are expected later in 2026 and may inform committees' scrutiny of the Scottish Budget 2027-28.
International examples
Other countries and governments are in a similar position to Scotland and are exploring ways to include prevention and health and wellbeing approaches in their decision-making and budgeting. Previously we mentioned how some of the principles which could enable prevention are outcome-based budgeting (see section Outcome-based resource allocation and accounting), and long-term thinking (see sections Prevention as a solution, and Change takes time). The international examples below show how different countries approach outcome-based budgeting. Outcome-based budgeting means making budget decisions based on how they contribute towards a government goal (i.e. tackling child poverty) rather than deciding how much money to allocate to each department.
While all countries shown below, like the Scottish Government, use a traditional portfolio-based budgeting method, they have managed to include some consideration for cross-departmental tracking of spending or activity towards government objectives. In this section we use information from Carnegie UK's Budgeting for Wellbeing: International Approaches.
 | The New Zealand Treasury required agencies to conduct a wellbeing analysis to show how their proposed spending contributed to wellbeing in the 2019 budget. The Public Finance (Wellbeing) Amendment Act required future government Fiscal Strategy Reports to explain how budget decisions align with wellbeing objectives. The Public Services Act (2020) further established interdepartmental executive boards, which oversee functions related to responsibilities of multiple departments. |
 | The Welsh Government's approach is centred around the Wellbeing of Future Generations (Wales) Act (2015), which makes it a statutory requirement for devolved public bodies to work towards the Welsh wellbeing goals. The Budget Improvement Plan (2024) uses the five ways of working (long-term, prevention, integration, collaboration, and involvement) to integrate this in the budgeting process. The Future Generations Commissioner and the Welsh Government use a Strategic Integrated Impact Assessment to review the Draft Budget annually to assess how it aligns with the Act, and to identify trends and cumulative impacts. |
 | In 2019, the Government of Iceland conducted a wide-scale public and expert consultation to identify six wellbeing priorities (Mental health, secure housing, better work-life balance, zero carbon emissions, increasing scale and intensity of innovation, better communication with the public) for the Government along with a set of key indicators. The Government then used these as a basis of its five-year fiscal strategy, which is aligned with annual budgets. The Prime Minister's Office is responsible for the wellbeing economy agenda. |
 | The Australian Early Intervention Investment Framework, run by the treasury of the state of Victoria directs funding towards initiatives using early intervention approaches, addressing issues before they get worse. The spending on early intervention policies has increased from 1% to 10% of new funding since 2021 and a growing number of initiatives requiring long-term financial commitments are being proposed and delivered. The development of this scheme followed a social impact bond, which Carnegie UK said "struggled to scale" initiatives. The new scheme is delivering on projected savings according to Carnegie UK. These savings are then kept in the fund and used to finance the upfront costs of further interventions, creating a positive reinforcement cycle. |
These examples present an alternative to more traditional ways of working by offering ways to link government outcomes to budget decisions, embed these outcomes in legislation (or build the legislation around these outcomes) and incentivise long-term strategic and fiscal planning. The most relevant to Scotland is perhaps the Welsh approach, where devolved powers were used to create new original legislation which makes it a requirement for public bodies to carry out sustainable development. Audit Wales conducted a review of lessons learned from the decade since the Wellbeing of Future Generations Act, which was accompanied by the Future Generations Commissioner's Future Generations Report 2025. Audit Wales makes recommendations for future work towards the Welsh wellbeing goals which are paraphrased below, and are relevant outside of the Welsh context:
Post-legislative evaluation and scrutiny: The Welsh Government should now clearly set out a scope and timetable for its own post-legislative evaluation and any changes to the [Wellbeing of Future Generations] Act.
Minimising uncertainty in funding: The Welsh Government faces its own constraints in setting longer-term budgets due to UK budget and political cycles. However, public bodies continue to describe the negative impact of annual settlements, late funding notifications, and in-year allocations. The Welsh Government should work with public bodies to explore and agree what can reasonably be done to minimise funding uncertainties and aid their medium and longer-term planning where possible.
Promoting prevention: The Commissioner has recommended that the Welsh Government ring-fences funding for prevention, which increases over time. This reflects calls from several organisations at a UK level. The Welsh Government should also explore other, complementary, ways of encouraging investment in prevention.
Understanding impact: The Welsh Government should work with public bodies to take a fresh look at the assessment of performance and impact under the Act. This work should consider how best to measure the impact public bodies are having and their contribution towards the wellbeing of Wales; and how assessment of performance and impact can promote the aims of the Act and reinforce the need to work preventatively and collaborate.
Wales, like Scotland, relies heavily on the block grant allocated from the UK Government through the Barnett Formula, meaning that it is impacted by the UK Budget and political cycles. Many of the points made by Audit Wales will therefore apply equally in a Scottish context, such as the need to minimise uncertainty. The points about post-legislative evaluation and scrutiny and about understanding the impact of the Wellbeing for Future Generations Act may not yet be relevant in Scotland , because there is no equivalent legislation. However, the principles of these two suggestions could be applied to the PSR Strategy or the NPF in a similar way.
Findings from expert consultations
Various organisations have approached Prevention from different points of view – public health, macroeconomics, accounting, auditing, inequalities to name just a few perspectives. In January and February 2026, we interviewed representatives CIPFA, SHERU, and from the OECD to ask them about their work on preventative spending in public bodies. We asked them what they saw as the main topic areas and challenges, and what the next steps could be to progress prevention from a goal and rhetoric, to practice. This section contains summaries of what they told us about their work.
The interview summaries shown in this section are not results of formal qualitative analysis and do not necessarily represent the views of SPICe or any of the consulted organisations. Instead, they are presented as summaries of conversations between SPICe researchers and representatives of these organisations.
CIPFA
CIPFA is an advocate for preventative spending to improve health and wellbeing in populations, and recent work has focused on changing the mindset on prevention and taking a whole-system view. This is important, considering that spending on prevention and feeling the benefits of doing so transcends the current portfolio-based government and budget structures used in UK administrations. CIPFA dedicates a section of its website to information about investment in prevention.
An ability to identify preventative spend would provide a foundation for better financial decision-making, increase transparency of preventative investment, and help to build the case for a greater emphasis on prevention i public finance. Previously, CIPFA worked with Public Health England (PHE) to propose a framework for evaluation of preventative investments. This provides a methodology for a balanced costs/benefits evaluation of financial and economic decision-making using a whole-system approach. This work highlighted the need for better understanding of current spending on prevention, using local assessment of public services or programmes as a pilot.
In 2023, CIPFA partnered with The Health Foundation on a project to explore the extent to which local authorities’ spending on preventative action (related to the wider determinants of health) could be quantified. The project included development of a ‘proof of concept’ model to track and identify preventative spend. Building on the findings of CIPFA's earlier work PHE, the project aimed to gain consensus on the definitions and scope for preventative action, and to map this against services/programmes and the associated levels of spending in partner councils.
Working with partner councils, CIPFA co-produced and tested a four-step approach that was designed to be adaptable across public sector organisations. CIPFA's Understanding Preventative Investment report, supported by The Health Foundation explained this approach and demonstrated for the first time that preventative investment can be defined, mapped and measured in financial terms. The report sets out guidance to enable public sector organisations to build a clearer picture of their levels of spend on prevention, alongside an adaptable mapping tool to provide a structure for recording and classifying services.
In our discussions with them, CIPFA highlighted that using traditional accounting methods to find out the current state of prevention spending is challenging. Quantifying spending on prevention requires the accountant to analyse spending based on its purpose, and is an objective-based exercise. By comparison, financial reports are traditionally structured around portfolios. In an approach which combines these, the same spending is effectively looked at twice, from different perspectives. One perspective gives a vertical view of the budget, looking top-down from the portfolio angle, and the other gives a horizontal perspective, looking at spending for a given purpose across all portfolios.
Put simply, a comparison of portfolio spending with prevention spending becomes meaningless because of the overlap between these classifications - when spending can be classed as both portfolio-based, and preventative, this inevitably leads to double counting. This doesn't mean that quantifying prevention is impossible. It just means that comparing preventative spending values to portfolio spending may not be as straightforward as one might think. CIPFA speculates that this has been one of the reasons why the Scottish Government's progress on reporting has been slower than committees would have liked or expected.
Another possible reason for slow progress on prevention which CIPFA highlights is the fragmented definitions of prevention, with everyone having different ideas of what it is. CIPFA says that it would be helpful for the Scottish Government and Scottish Parliament to agree on a shared understanding of prevention, across parties and departments, and to determine the nature of the baseline they want to create and how it may be useful to them. Despite best efforts, CIPFA warns that there is likely to always be a level of subjectivity when tagging a budget for preventative spending.
Moving forward, CIPFA contacts explained that the organisation planned to keep working with The Health Foundation, specifically on addressing how to make the shift towards prevention, and how to identify and evaluate investment. This would build on the work to date to support identification of preventative spend, and would also consider the process of decision-making and evaluation of preventative investment. In addition to this, CIPFA planned to conduct work focusing on some of the challenges associated with prevention, as well as continuing policy work on how prevention is key to public sector reform and sustainability across the UK.
SHERU
Between FAI and the Strathclyde Centre for Health Policy sits SHERU, a research unit focused on providing evidence and insight on health inequalities in Scotland. As part of its work, the Unit publish a regular Prevention Watch round-up, which updates on the use of prevention as a means of public service delivery to reduce health inequalities.
SHERU's take was that good definitions of prevention already exist. SHERU uses the same definition as Public Health Scotland, but our interviewees suggested that any definition used would be good as long as it was consistent across departments, the Parliament and all public service delivery bodies. Letting perfection stand in the way of a good thing would be a mistake here, and SHERU was of the opinion that it was probably time to move on from defining what prevention is. Instead, the Government should be focused on using existing definitions and tools to conduct analyses and create a way to use the results in future policy making and budgeting activities.
To make this happen, SHERU suggested that the Scottish Government should be clear about what it is that it is trying to prevent from happening. The definition of prevention is not that difficult to grasp as a concept – keep a bad thing from happening instead of correcting the impacts of the bad thing. However, the meaning changes based on what the bad thing is. This has accounting implications. A prevention tagging exercise could produce different results based on what is being prevented. An activity which prevents demand for social security payments might not prevent there being demand for hospitalisations due to cardiovascular problems. SHERU felt that the Scottish Government should provide more information on what it was trying to prevent, and make sure this was aligned with its goals. A vehicle for this could be the National Performance Framework, where the Scottish Government could use to set clear targets and inform budget-holders on what they should be preventing, thus formulating strategic outcomes for Scotland. Increased clarity on this would also help with the issue of all spending being potentially classifiable as “prevention”.
During the interview, SHERU also mentioned the structure of Scottish Parliament committees, and how the structure used in Session 6 of the Parliament, which mirrored Government portfolios, was not very compatible with carrying out budget scrutiny from a preventative perspective. Subject committees don't always consider the financial aspects of the policies they scrutinise in inquiries. Instead, they focus on questions relating directly to their portfolio and leave Budget scrutiny to the Finance and Public Administration Committee. This creates a mode of working which can become siloed. In some cases, this can be compounded with a varying level of financial literacy across committees, creating a situation where a subject committee fails to consider the financial implications of its recommendations and legislative amendments. Encouraging outcome-based committee work, whole-of-Parliament discussion, and cross-committee work could help this situation.
The same silo problem propagates to scrutiny from the Scottish Government's perspective. It is very difficult for any Cabinet Secretary to answer questions about prevention-related policy and spend if it falls outwith their department. So, for example if talking about spending on improving housing, the preventative spending action might lie with the Cabinet Secretary for Housing, but the effects of reduced demand for reactive treatment of respiratory disease will lie with the Cabinet Secretary for Health and Social Care. Logically, this is fine – both Cabinet Secretaries work to improve people's lives, but cross-departmental scrutiny is not common practice, and clearly preventative approaches require it to gain a full understanding of the impact of spending decisions. SHERU suggested that to address this, it might be useful to encourage whole-of-parliament discussions and outcome-based committee work. In our discussion with SHERU, we also talked about the potential to improve cross-government scrutiny by changing the structure of Scottish Parliament committees, or adding a committee dedicated to cross-portfolio activity be established.
SHERU researchers felt that scrutiny should ideally be combined with governance and deliverability of outcomes. If prevention is to be used as a tool for setting budgets, the responsibility for incorporating prevention into the budget making process needs to lie with the people responsible - in this case, the Scottish Government, and specifically the Cabinet Secretary for Finance and Local Government. This would require buy-in and effort at a Ministerial level, however it might be the only way to progress prevention from a talking point and a reported statistic to a principle used in allocating resources.
OECD
The OECD health division collects and reports on health statistics and financing from partner countries and publishes work on the economics of health, including spending on prevention. This includes reports such as the Fiscal Sustainability of Health Systems or the periodical Health at a Glance series, which has a subsection on health expenditure. Prevention spending is published within the Health expenditure and financing dataset. Data for the UK is provided as an aggregate of all UK nations, meaning that Scotland is not covered in its own right. Spending on prevention makes up around 3% of health expenditure for most OECD nations. There is a critical limiting factor to this data: it only covers prevention within the healthcare budget. In this briefing we have shown, however, that prevention transcends budget portfolios.
Comparing preventative spending across countries becomes tricky due to a familiar issue: different countries having slightly different definitions of what they consider prevention. For data to be accurate, it would have to be collected using a standardised way, with fidelity of cost centres across thousands of local authority budgets. There is in theory a standardised way - the OECD System of Health Accounts 2011 provides detailed guidance on what should be considered prevention and categorises healthcare expenditure activities to make prevention accounting possible within healthcare budgets. However, this still doesn't get around the problem of being limited to the realm of the healthcare spending portfolio and not capturing cross-departmental effects of preventative spending. So far, no country has published a spending review which would make it possible to present prevention spending across departments.
OECD contacts also highlighted the need to measure the effectiveness of preventative spending. This includes curating a list of key indicators; for instance, indicators like breast cancer screening rates, or vaccination rates are used to measure how much prevention is being done. One would expect increased spending on prevention to lead to higher screening and vaccination rates, but this proposition should be carefully studied to make sure the money is being spent efficiently.
OECD researchers explained that their next step was to work out how spending on prevention might be protected. During recent times of austerity and following the financial crash of 2008, spending on prevention, such as screening programmes, has taken a hit, contributing to the problems the healthcare sector is facing today. The OECD is looking at how prevention spending might be financed, and how this financing could be protected. It is likely that any suggestions the OECD makes on best practice for administrations will involve some degree of ring-fencing, but other options exist, as shown with the international examples we set out.
Conclusions and next steps
In this briefing, we have presented the situation in public services, which are strained under very high levels of demand. Many public service providers are facing financial difficulties, with some already at risk of not being able to fulfil their statutory duties. We have presented some of the causes of this situation, focussing on the demographic change in Scotland, and how this influences demand for public services and their funding.
We presented evidence which points to a shift to preventative approaches as a potential solution to the challenges faced. This would involve focusing on funding and policy which facilitate approaches which reduce risk factors, promote building blocks of health, and focus on improving people's wellbeing and health, as well as preventing problems from happening. The evidence we set out introduces preventative approaches as an alternative to the current system, where large amounts of funding are dedicated to responding to problems which could have been prevented from appearing in the first place.
The Scottish Parliament and its committees, The Scottish Government, NGOs, think tanks, and other organisations in the UK and elsewhere are trying to come up with ways to make public services financially sustainable in the long-term, and many of their propositions include preventative approaches. We showed some of the work being done in Scotland and abroad, with the most important policy to date being the Public Service Reform Strategy, the National Performance Framework, and various strategies for modernisation of individual public services. In addition to this, The Scottish Government is piloting an approach for tagging preventative spending across the Scottish Budget, with results of this pilot expected to be published later in 2026.
The outcomes of The Scottish Government's budget-tagging pilot will be critical for determining the direction of action around the shift to preventative approaches in future policy and funding allocations. Once there is a baseline figure for preventative spending, there is an expectation that the Scottish Government will be better able to formulate plans to develop it further and work towards delivering its policy objectives from the National Performance Framework and other documents. To make this effective, experts told us that the Scottish Government should make it very clear what it is trying to prevent, and what it means by prevention.
The next steps after this could involve both the Scottish Government and the Scottish Parliament considering how they might enable cross-departmental scrutiny of all-of-government objectives. We have presented some international examples of how this has been done elsewhere, including a very relevant example from Wales. The evidence in this briefing suggests potential ways of achieving this might be through outcome-based budgeting, where money is allocated to a goal rather than a department, through potential new legislation, or even through setting up of dedicated cross-departmental units or committees which would oversee work that spans multiple Government departments.
It is possible that prioritising preventative approaches from a budgetary point of view will require a change to the way budgets are allocated. This could involve changing the time-frames for setting and scrutinising budgets, linking budgets more clearly to outcomes, making better use of cross-portfolio impact assessments, ring-fencing spending on prevention, or including a way to calculate the real costs of policies, to name just a few approaches.
A key opportunity to progress the use of preventative approaches to in Scotland will emerge with the results of the Scottish Government's budget-tagging pilot, and the reaction and subsequent action of both the Government and wider public sector to the findings. Scrutiny of how the Government progresses with this work by both the Parliament and wider stakeholders is also a significant opportunity to progress and promote the preventative agenda.
Monitoring the preventative landscape is likely to be a priority for the new committees of the Scottish Parliament in Session 7, and they will not be short of sources. Over the past 18 months, Demos and The Health Foundation published the two following reports, in addition to the one discussed in this briefing:
Counting what matters: How to classify, account and track spending for prevention
The Preventative Shift: How can we embed prevention and achieve long term missions.
More contributions can be expected from the sources mentioned in this briefing here, as well as others like the Scottish Prevention Hub at the Edinburgh Futures Institute, or the Royal Society, which published the report The shift to prevention: A new ecosystem of health promotion and protection in June 2025. Keeping up with the news on prevention might get tricky in the near future, with so many organisations involved, so for Scotland sources such as Prevention Watch will remain valuable. Other organisations will no doubt continue to contribute to the preventative agenda, for instance Scottish Futures Trust's publication on long-term infrastructure for Scotland has a heavy focus on cross-cutting prevention-based approaches.
Demos had previously set a tough challenge, proposing the UK rebuilds itself into a Preventative State:
The system breaks down through the sheer weight of demand. In failing to deliver for citizens in their moment in need, we break the bonds of trust that are essential for society to function. Our society, our economy and our democracy are significantly weakened.
So we urge something entirely more ambitious: a fundamental re-conception of the role of the state from plugging the gaps in people's lives and mopping up when things go wrong, to building stronger communities, where a rich social fabric reverses the societal fragmentation that is the silent driver of so much demand on public services.
As Session 7 of the Scottish Parliament approaches, time will tell how the next Scottish Government responds to the challenges of fully embracing a preventative agenda.
Acronyms
| Abbreviation | Meaning |
|---|---|
| BBH | Building Block of Health |
| CCP | Climate Change Plan |
| CDEL | Capital Department Expenditure Limit |
| CIPFA | Chartered Institute for Public Finance and Accountancy |
| COSLA | Convention of Scottish Local Authorities |
| FAI | Fraser of Allander Institute |
| FPAC | Finance and Public Administration Committee |
| GDP | Gross Domestic Product |
| IJB | Integration Joint Board |
| LEZ | Low Emissions Zone |
| LGIU | Local Government Information Unit |
| NPF | National Performance Framework |
| OECD | Organisation for Economic Co-operation and Development |
| PDEL | Preventative Department Expenditure Limit |
| PHE | Public Health England |
| PHF | Population Health Framework |
| PHS | Public Health Scotland |
| PSR | Public Service Reform |
| QALY | Quality-Adjusted Life Year |
| RCP | Royal College of Physicians |
| RDEL | Resource Department Expenditure Limit |
| SFC | Scottish Fiscal Commission |
| SHERU | Scottish Health Equity Research Unit |
| SIMD | Scottish Index of Multiple Deprivation |
| WEMWBS | Warwick-Edinburgh Mental Wellbeing Scale |
| WHO | World Health Organization |
Sources
Roy, G., Ryan, E., & Riccomini, J. (2026, February 25). Fiscal Sustainability Perspectives: what Scotland’s finances mean for the next parliament. Retrieved from <a href="https://fiscalcommission.scot/publications/fiscal-sustainability-perspectives-what-scotlands-finances-mean-for-the-next-parliament-february-2026/" target="_blank">https://fiscalcommission.scot/publications/fiscal-sustainability-perspectives-what-scotlands-finances-mean-for-the-next-parliament-february-2026/</a> [accessed 4 March 2026]
Ipsos. (2023). Scottish Household Survey Data Explorer. Retrieved from <a href="https://scotland.shinyapps.io/sg-scottish-household-survey-data-explorer/" target="_blank">https://scotland.shinyapps.io/sg-scottish-household-survey-data-explorer/</a> [accessed 20 February 2026]
Office for National Statistics. (2025, December 10). Published data related to life expectancies. Retrieved from <a href="https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/datalist?filter=datasets" target="_blank">https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/datalist?filter=datasets</a> [accessed 20 February 2026]
Scottish Government. (2022). Attitudes to family formation in Scotland. Retrieved from <a href="https://www.gov.scot/publications/attitudes-family-formation-scotland/" target="_blank">https://www.gov.scot/publications/attitudes-family-formation-scotland/</a> [accessed 19 February 2026]
Office for National Statistics. (2025, December 10). Published data related to life expectancies. Retrieved from <a href="https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/datalist?filter=datasets" target="_blank">https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/datalist?filter=datasets</a> [accessed 19 February 2026]
Office for National Statistics. (2015, September 9). How has life expectancy changed over time?. Retrieved from <a href="https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/articles/howhaslifeexpectancychangedovertime/2015-09-09" target="_blank">https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/articles/howhaslifeexpectancychangedovertime/2015-09-09</a> [accessed 18 February 2026]
Feeley, D. (2021, February 3). Independent Review of Adult Social Care in Scotland. Retrieved from <a href="https://www.gov.scot/publications/independent-review-adult-social-care-scotland/pages/0/" target="_blank">https://www.gov.scot/publications/independent-review-adult-social-care-scotland/pages/0/</a> [accessed 5 March 2026]
Picken, A. (2025, December 3). Seven health boards given £230m bailout loans despite record funding. Retrieved from <a href="https://www.bbc.co.uk/news/articles/cde62x6dy01o#:~:text=Bailout%20loans%20received%20by%20NHS%20boards&text=The%20loans%20system%20was%20suspended,by%20boards%20in%202024%2F25." target="_blank">https://www.bbc.co.uk/news/articles/cde62x6dy01o#:~:text=Bailout%20loans%20received%20by%20NHS%20boards&text=The%20loans%20system%20was%20suspended,by%20boards%20in%202024%2F25.</a> [accessed 6 March 2026]
Public Health England. (2018, September 11). Health profile for England: 2018. Retrieved from <a href="https://www.gov.uk/government/publications/health-profile-for-england-2018" target="_blank">https://www.gov.uk/government/publications/health-profile-for-england-2018</a> [accessed 5 March 2026]
National Records for Scotland. (2024). Life Expectancy in Scotland 2021-23. Retrieved from <a href="https://www.nrscotland.gov.uk/publications/life-expectancy-in-scotland-2021-2023/" target="_blank">https://www.nrscotland.gov.uk/publications/life-expectancy-in-scotland-2021-2023/</a> [accessed 6 March 2026]
Office for National Statistics - Demography team. (2025, December 10). National life tables – life expectancy in the UK: 2022 to 2024. Retrieved from <a href="https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/bulletins/nationallifetablesunitedkingdom/2022to2024" target="_blank">https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/bulletins/nationallifetablesunitedkingdom/2022to2024</a> [accessed 12 February 2025]
Roy, G., Ryan, E., & Riccomini, J. (2025). Fiscal Sustainability Report. Retrieved from <a href="https://fiscalcommission.scot/publications/fiscal-sustainability-report-april-2025/" target="_blank">https://fiscalcommission.scot/publications/fiscal-sustainability-report-april-2025/</a> [accessed 16 February 2026]
Robertson, F.J. (1944). Rising Costs in Running City. Edinburgh Evening News.
Johnston, L., Milligan, B., Miller, N., Allan, M., Dorian, C., & Calder, C. (2025, December 4). NHS in Scotland 2025: Finance and performance. Retrieved from <a href="https://audit.scot/publications/nhs-in-scotland-2025-finance-and-performance" target="_blank">https://audit.scot/publications/nhs-in-scotland-2025-finance-and-performance</a> [accessed 10 February 2026]
McClelland, C., Holgate, C., Sibbald, K., & Blyth, D. (2026, February 26). Integration Joint Boards Financial bulletin 2024/25. Retrieved from <a href="https://audit.scot/publications/integration-joint-boards-finance-bulletin-202425" target="_blank">https://audit.scot/publications/integration-joint-boards-finance-bulletin-202425</a> [accessed 3 March 2026]
Dickson, N. (1998, July 1). The NHS: 'One of the greatest achievements in history'. Retrieved from <a href="http://news.bbc.co.uk/1/hi/events/nhs_at_50/special_report/123511.stm" target="_blank">http://news.bbc.co.uk/1/hi/events/nhs_at_50/special_report/123511.stm</a> [accessed 2 March 2026]
Hoddinott, S., Fright, M., & Pope, T. (2022, October 25). 'Austerity' in public services: lessons from the 2010s. Retrieved from <a href="https://www.instituteforgovernment.org.uk/publication/report/austerity-public-services-lessons-2010s" target="_blank">https://www.instituteforgovernment.org.uk/publication/report/austerity-public-services-lessons-2010s</a> [accessed 17 February 2026]
Public Health Scotland. (2026, January 26). Public approach to prevention: The building blocks of health. Retrieved from <a href="https://publichealthscotland.scot/about-us/what-we-do-and-how-we-work/public-health-approach-to-prevention/the-building-blocks-of-health/#:~:text=Unfair%20differences%20in%20income%2C%20wealth,need%20to%20be%20in%20place." target="_blank">https://publichealthscotland.scot/about-us/what-we-do-and-how-we-work/public-health-approach-to-prevention/the-building-blocks-of-health/#:~:text=Unfair%20differences%20in%20income%2C%20wealth,need%20to%20be%20in%20place.</a> [accessed 9 February 2026]
Public Health Scotland. (2026). Together we can: Our 10-year strategy to 2035. Retrieved from <a href="https://publichealthscotland.scot/about-us/what-we-do-and-how-we-work/together-we-can-our-10-year-strategy-to-2035/scotland-s-health-now/impact-economy-and-threats/" target="_blank">https://publichealthscotland.scot/about-us/what-we-do-and-how-we-work/together-we-can-our-10-year-strategy-to-2035/scotland-s-health-now/impact-economy-and-threats/</a> [accessed 10 February 2026]
Tinson, A. (2020, July). Living in poverty was bad for your health long before COVID-19. Retrieved from <a href="https://www.health.org.uk/reports-and-analysis/briefings/living-in-poverty-was-bad-for-your-health-long-before-covid-19" target="_blank">https://www.health.org.uk/reports-and-analysis/briefings/living-in-poverty-was-bad-for-your-health-long-before-covid-19</a> [accessed 10 February 2026]
Scott, Z., & Roy, E. (2025). Understanding preventative investment. Retrieved from <a href="https://www.cipfa.org/-/media/files/policy-and-guidance/health-and-wellbeing/understanding-preventative-investment.pdf" target="_blank">https://www.cipfa.org/-/media/files/policy-and-guidance/health-and-wellbeing/understanding-preventative-investment.pdf</a> [accessed 15 January 2026]
Brand, C., & Hunt, A. (2018, May 18). The health costs of air pollution from cars and vans. Retrieved from <a href="https://www.cleanairday.org.uk/files/the_health_costs_of_air_pollution_from_cars_and_vans_20180518.pdf" target="_blank">https://www.cleanairday.org.uk/files/the_health_costs_of_air_pollution_from_cars_and_vans_20180518.pdf</a> [accessed 9 February 2026]
Garett, H., Mackay, M., Nicol, S., Piddington, J., & Roys, M. (2021). The cost of poor housing in England. Retrieved from <a href="https://files.bregroup.com/research/BRE_Report_the_cost_of_poor_housing_2021.pdf" target="_blank">https://files.bregroup.com/research/BRE_Report_the_cost_of_poor_housing_2021.pdf</a> [accessed 11 February 2026]
Walker, S. (2023, September 10). Investing in breath: the true cost of lung conditions to the UK economy. Retrieved from <a href="https://www.asthmaandlung.org.uk/blog/campaigning/investing-breath-true-cost-lung-conditions-uk-economy" target="_blank">https://www.asthmaandlung.org.uk/blog/campaigning/investing-breath-true-cost-lung-conditions-uk-economy</a> [accessed 10 February 2026]
Brooke, A. (2022). Respiratory Disease: understanding the future service and workforce needs . Retrieved from <a href="https://www.hee.nhs.uk/sites/default/files/documents/Respiratory%20Disease%20Report.pdf" target="_blank">https://www.hee.nhs.uk/sites/default/files/documents/Respiratory%20Disease%20Report.pdf</a> [accessed 10 February 2026]
Trueman, D., Woodcock, F., & Hancock, E. (2017). Estimating the economic burden of respiratory illness in the UK. Retrieved from <a href="https://www.asthmaandlung.org.uk/economic-burden-report" target="_blank">https://www.asthmaandlung.org.uk/economic-burden-report</a> [accessed 10 February 2026]
Lent, A. (2025, July 21). Doing With: reinventing public services in a time of crisis. Retrieved from <a href="https://www.kingsfund.org.uk/insight-and-analysis/long-reads/doing-with-reinventing-public-services-time-crisis" target="_blank">https://www.kingsfund.org.uk/insight-and-analysis/long-reads/doing-with-reinventing-public-services-time-crisis</a> [accessed 12 February 2026]
Martin, S., Lomas, J., & Claxton, K. (2020). Is an ounce of prevention worth a pound of cure? A cross-sectional study of the impact of English public health grant on mortality and morbidity. BMJ Open. doi: 10.1136/bmjopen-2019-036411
Wimalasena, N.N., Chang-Richards, A., Wang, K.I.K., & Dirks, K.N. (2021). Housing Risk Factors Associated with Respiratory Disease: A Systematic Review. International Journal of Environmental Research and Public Health. doi: 10.3390/ijerph18062815
National Institute for Health and Care Excellence. (2025, December 1). Changes to NICE’s cost-effectiveness thresholds confirmed. Retrieved from <a href="https://www.nice.org.uk/news/articles/changes-to-nice-s-cost-effectiveness-thresholds-confirmed" target="_blank">https://www.nice.org.uk/news/articles/changes-to-nice-s-cost-effectiveness-thresholds-confirmed</a> [accessed 19 February 2026]
ICER. (n.d.) Cost-Effectiveness, the QALY, and the evLY. Retrieved from <a href="https://icer.org/our-approach/methods-process/cost-effectiveness-the-qaly-and-the-evlyg/" target="_blank">https://icer.org/our-approach/methods-process/cost-effectiveness-the-qaly-and-the-evlyg/</a> [accessed 19 February 2026]
Taylor, M., & Filby, A. (2015). PRM40 - Are Qalys An Appropriate Measure To Use When Evaluating Public Health Interventions In The Uk?. Value in health. doi: 10.1016/j.jval.2015.09.2556
Sawhney, T.G., Dobes, A., & O'Charoen, S. (2023). QALYs: The Math Doesn’t Work. Journal of Health Economics and Outcomes Research, 10-13. doi: 10.36469/001c.83387