The impact of cash transfers in the first 1000 days on child health outcomes and health inequalities: an evidence review
This briefing presents findings from research undertaken as part of an Academic Fellowship between October 2025 and March 2026. Emma Stewart (University of Glasgow) explores the international evidence for payments in the prenatal and postnatal period. In Scotland, these payments include the Best Start Grant.
Summary
The first 1000 days – from conception to age two – are a critical window for shaping a child's lifelong health and development. Growing up in poverty can harm a child's health, starting before birth and continuing through their physical, emotional, and mental development. Research from both rich and poor countries shows that giving cash directly to mothers during pregnancy and in the early years of a child's life can lead to better health outcomes – like fewer premature births, lower chances of dying in infancy, healthier birth weights, better breastfeeding rates, and more use of health services.
Cash transfers in the early years have become a widely used policy lever to support families with young children and reduce socio-economic inequalities. Cash transfers are regarded as an investment in human capital across the life course. A large body of evidence demonstrates that increasing family income and reducing material deprivation can improve birth outcomes, support child health, and help break intergenerational cycles of disadvantage, yet we still lack understanding of what policy features are most important for reducing child health inequalities.
This evidence review focuses specifically on cash transfers designed to support families during pregnancy and early childhood, a key period when health inequalities begin to emerge. By synthesising evidence on the health impacts of cash transfers – including one-off and regular payments – the study assesses how income support in the prenatal and early postnatal period influences child health outcomes, with particular attention to causal pathways, policy design features, and implications for reducing health inequalities.
Key findings include:
One-off lump sum payments delivered during pregnancy consistently improve birth outcomes but tend to have mixed or modest effects in the postnatal period.
Most policies effective at improving child health are unconditional, recurring, and targeted at low-income families or delivered universally in high-poverty areas.
Evidence is lacking for the impact of one-off and regular payments on child health or development beyond infancy.
Cash transfers during pregnancy and early childhood may potentially reduce child health inequalities but more research evidence is needed.
These patterns remain consistent across Australia, Canada, Poland, South Korea, Spain, Switzerland, US and UK.
Section 1: Introduction
A good start in life, beginning before conception and continuing through pregnancy and infancy, lays the foundation for health, development and well-being across the life course12. Early life experiences shape biological development, influence cognitive and socio-emotional outcomes, and have lasting effects on the risk of chronic disease and health inequalities in adulthood34. Giving every child the best start in life is a priority for reducing health inequalities5.
Despite high overall living standards, material deprivation during the early years remains a significant driver of unequal outcomes in high-income countries. Financial constraints during pregnancy and infancy can affect nutrition, housing security and parental stress, with implications for both maternal and child health.
Understanding the extent to which cash-based interventions improve child health outcomes, and reduce health inequalities, is essential to inform policy design and ensure that public spending delivers maximum benefit during this formative period.
1.1 Family income and pathways to child health outcomes
A significant body of research shows that increases in family income and reductions in poverty are associated with improvements in child health and development. Since 2018, several systematic and scoping reviews have documented consistent positive associations between higher family income (including cash transfers) and a range of maternal and child health outcomes1234567. This work suggests that even relatively modest income increases in early life can have lasting effects on health and human capital.
Cash transfers operate through a set of well-established causal pathways that directly or indirectly link family income to child outcomes4. The investment model emphasises that increased income improves material conditions, enabling families to invest in healthcare, housing, and cognitively enriching activities, while the parental stress model highlights reductions in financial strain that support better parental mental health and more responsive parenting.
These pathways vary across the different stages of early childhood, from pregnancy to pre-school. For example, cash transfers at birth may facilitate care-giving behaviours such as breastfeeding and skin-to-skin care, which are known to improve infant outcomes. During infancy, cash transfers can improve health directly by increasing parental investment in nutrition, housing and essential goods, while indirectly reducing parental stress and associated unhealthy behaviours like smoking. In early childhood, cash transfers enable families to establish healthy routines and invest in supportive home environments while simultaneously reducing parental stress and increasing quality time with children.
Cash transfers that are conditional on engagement with antenatal and postnatal services is another key pathway to influence child health. Payments that encourage earlier and more regular antenatal attendance mean that healthcare providers can detect complications such as pre-eclampsia, provide guidance on healthy behaviours, and facilitate interventions that improve maternal and infant outcomes.
The introduction or removal of cash payments can also prompt behavioural change. In the short run, policy implementation can influence the timing of births through either delaying pregnancies or adjusting planned delivery. Advancing or postponing birth can affect newborn health by altering the time available for fetal development.
Through these pathways – greater parental investment, reduced stress and improved access to health services– cash transfers can contribute to better short- and long-term child health and development outcomes.
1.2 Health inequalities and targeted early years interventions
Health inequalities emerge early in life and often persist across the life course. Differences in birth and child health outcomes, such as low birthweight, prematurity, and early developmental delays, are closely linked to socio-economic status, with children from more deprived families consistently experiencing worse outcomes. These early divergences can shape educational attainment, labour market prospects, and long-term health, reinforcing the intergenerational transmission of disadvantage.
Cash transfers that target vulnerable households during pregnancy or early childhood can mitigate some of these disparities. Several studies in high-income countries demonstrate that financial support to low-income families can improve birth outcomes, infant health, and child development12345. Such policies not only improve immediate health and well-being but may also interrupt the cycle of poverty, making the study of inequalities a key part of research on cash transfers6.
1.3 Evidence gaps and research needed
Building upon an expanding evidence base, including the aforementioned systematic reviews and evaluations of Best Start Grant1 and the Five Family Payments2 in Scotland, more research is needed to clarify the causal impacts of poverty reduction during early childhood. Evidence is required to determine which policy elements have the greatest effect on child health inequalities.
This review addresses critical gaps in the literature by synthesising evidence on cash transfers delivered during the first 1,000 days of life in high-income countries. Unlike previous work, it explicitly considers conditionality, targeting, and the potential to reduce health inequalities, providing a nuanced understanding of how design features influence outcomes. By integrating these factors, the briefing offers insights to support the optimal design of interventions that promote child health and equity.
1.4 Scope of the review
The evidence review addresses the following:
1. What are the effects of cash transfers received in the first 1000 days on child health outcomes, in high income countries?
2. How do policy features like targeting and conditionality influence child health outcomes and inequalities?
1.5 Report structure
Section 2 provides background information on cash transfer policies in Scotland and other high-income countries.
Section 3 outlines findings on the impact of one-off cash transfers in the first 1000 days on child health outcomes.
Section 4 outlines findings on the impact of regular cash transfers in the first 1000 days on child health outcomes.
Section 5 examines evidence on the impact of cash transfers on child health inequalities.
Section 6 summarises key findings and insights from the evidence review.
The evidence search and analysis is described in Appendix A1 with summary findings presented in Tables A1-2.
1.6 About the author
Emma Stewart is Research Associate in Public Health, School of Health and Wellbeing at the University of Glasgow. Emma has expertise in understanding social policies to improve child and maternal health.
Emma has been working with the Scottish Parliament Information Centre (SPICe) as part of its Academic Fellowship programme. This aims to build links between academic expertise and the work of the Scottish Parliament.
Any views expressed in this briefing are those of the author and do not necessarily represent those of SPICe or the Scottish Parliament.
1.7 Acknowledgements
Special thanks to the SPICe team and Camilla Kidner for her guidance and support. Thanks also to colleagues at the University of Glasgow for input on design, critical appraisal, and reviewing earlier drafts.
This work was funded by the Medical Research Council Impact Acceleration Account (MRC – IAA), with support for travel costs from the Economic and Research Council Impact Acceleration Account (ESRC IAA).
1.8 List of figures and tables
Figure 1: Cash transfers in pregnancy and early childhood - Scotland (2000-2026)
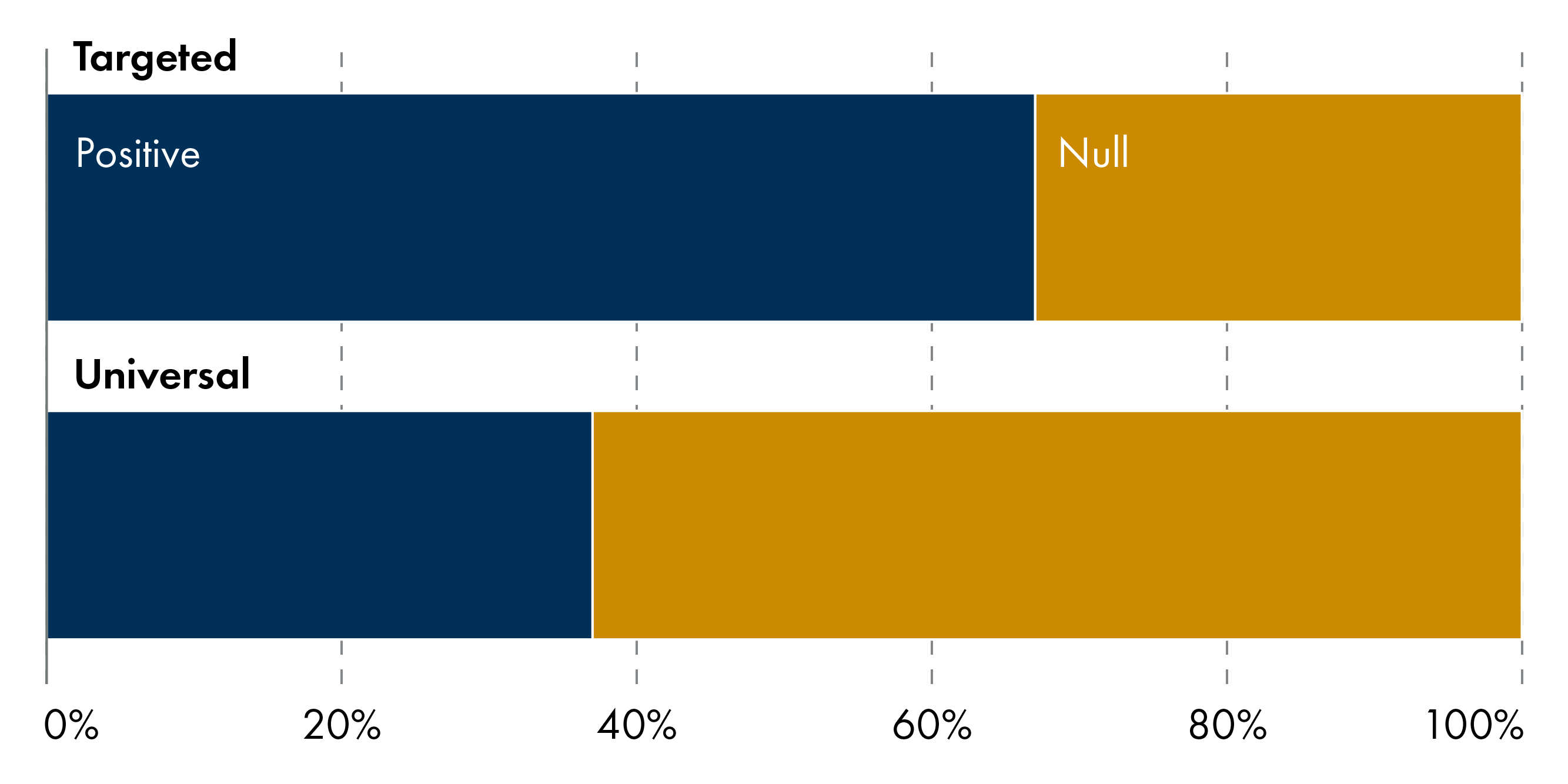
Figure 2: Universal and targeted one-off cash transfers by early years outcomes (n=65)
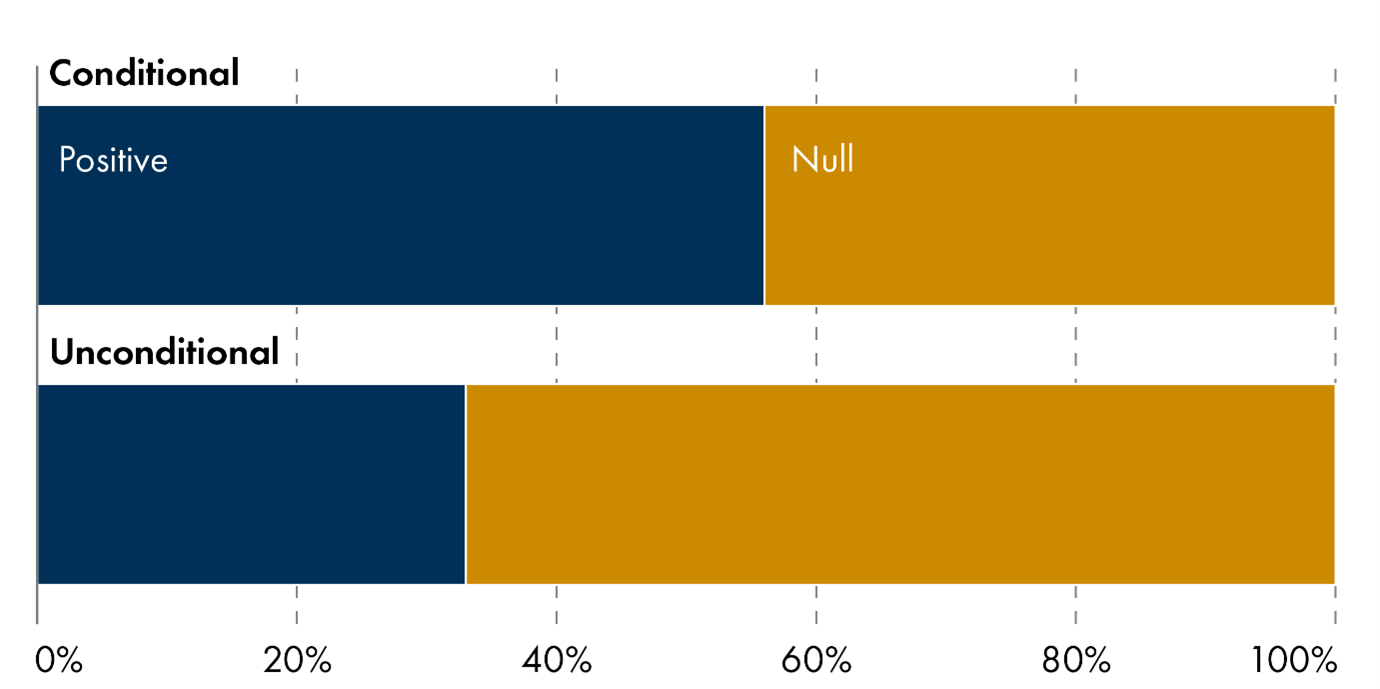
Figure 3: Unconditional and conditional one-off cash transfers by early years outcomes (n=63)
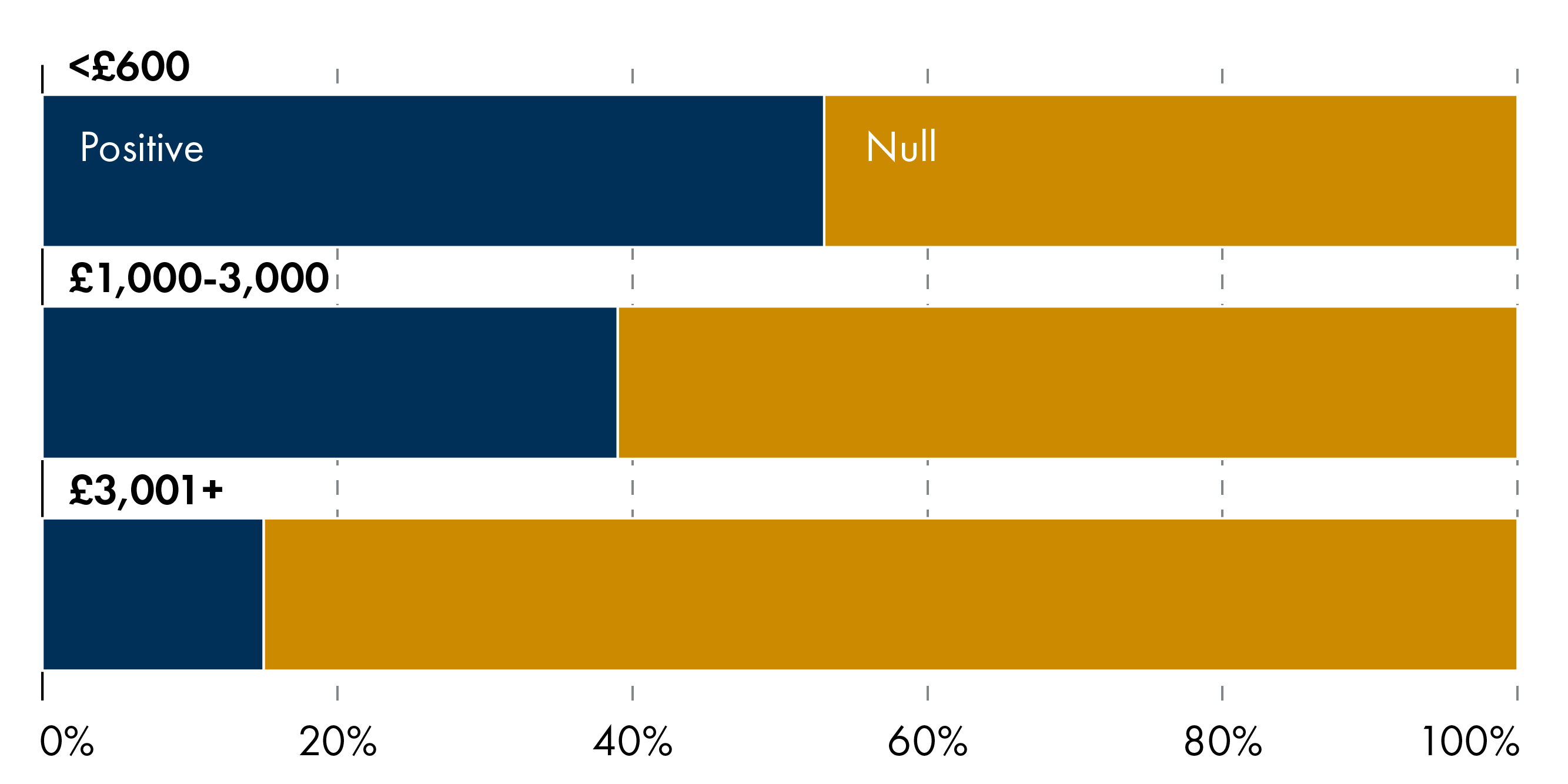
Figure 4: Payment size of one-off cash transfers by early years outcomes (n=65)
Figure 5: Evidence on one-off cash transfers by early years outcomes and study quality (n=55)
Figure 6: Payment size of regular cash transfers by early years outcomes (n=73)
Figure 7: Evidence on regular cash transfers by early years outcomes and study quality (n=63)
Figure 8: Summary of positive child health outcomes by policy targeting and conditionality (n=143/138)
Figure 9: Summary of studies reporting positive child health outcomes (N=27)
Table A1: Summary of findings – one-off cash transfers in first 1000 days (n=13)
Table A2: Summary of findings – regular cash transfers in first 1000 days (n=14)
Table A3: Key policy features of early years cash transfers in high income countries (N=11)
Section 2: Policy background
2.1 Early years cash transfers in Scotland and UK
The first 1,000 days have been prioritised by UK policymakers in several high-level strategy documents1234. A range of policies have been implemented to improve pregnancy and early years outcomes, including cash transfers delivered at or around birth. These take different forms including one-off baby bonuses, regular payments, social security benefits, and in-kind support; some are targeted to low-income families/mothers while others are universal.
Welfare payments specifically targeting women during pregnancy have existed in the UK for over 30 years. One off payments have included a Maternity Payment (1986; £80), Sure Start Maternity Grant (SSMG) (2000 – present; £500) and the Health in Pregnancy Grant (HiP) (2009-2011; £190).
Scotland has a distinct package of Five Family Payments that provides early years financial support including one off and regular payments. In 2018, Scotland replaced the SSMG with the Best Start Grant (BSG). This means tested grant comprises three one-off payments: Pregnancy and Baby Payment (£796 for first child; £398 for subsequent children); Early Learning Payment (£331 per child aged 2 to 3½ years); School Age Payment (£331 per child). The Scottish Child Payment (SCP) (£28 per child weekly) provides ongoing financial support throughout early childhood and beyond. A summary of early years cash transfers in Scotland is shown in Figure one.
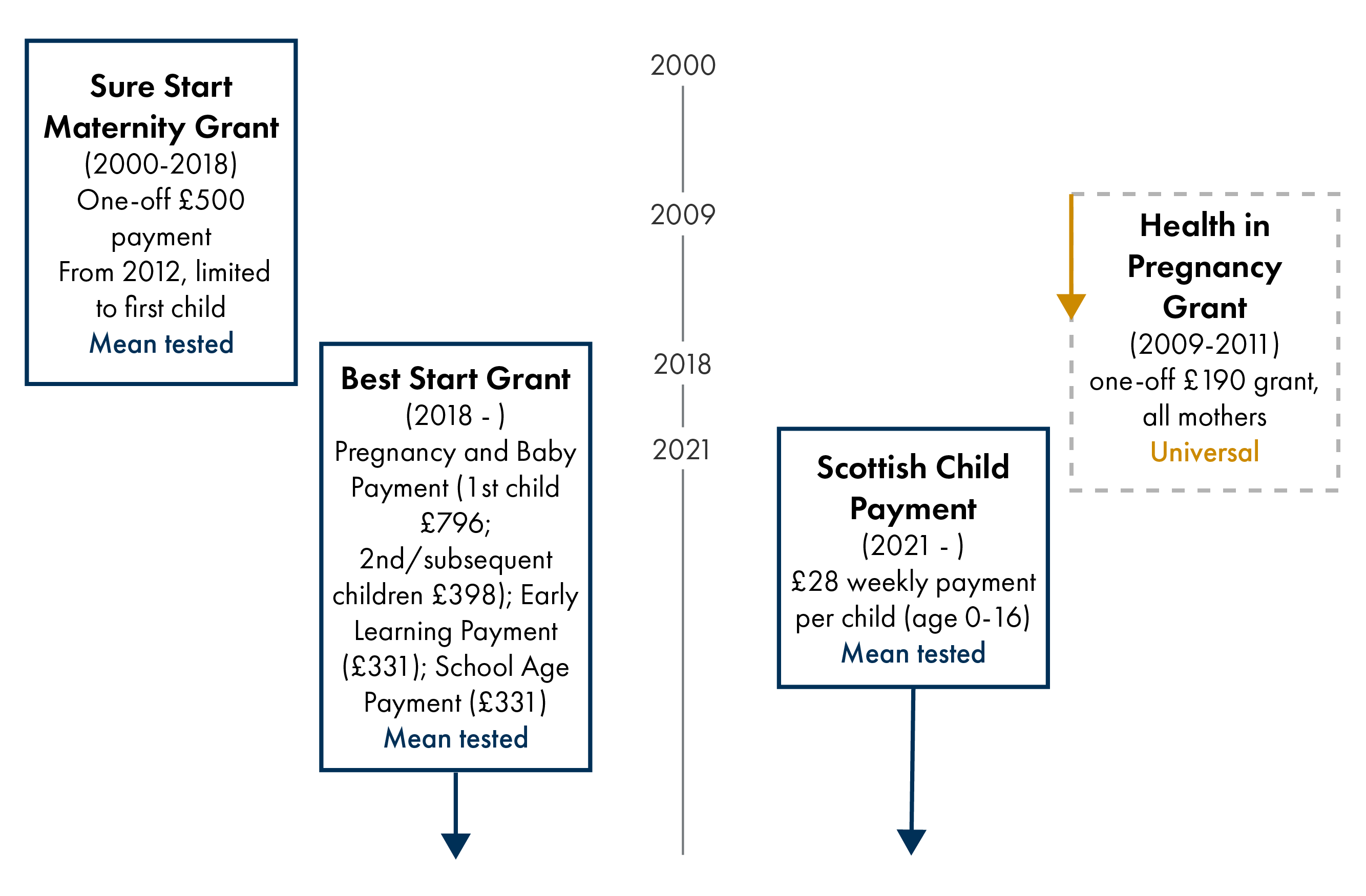
Adapted from Stewart, E. (2022). Welfare Grants in Pregnancy and Early Childhood. MatCHNet Policy Report 1, University of Glasgow. Retrieved from https://eprints.gla.ac.uk/270469/
2.2 Early years cash transfers in high income countries
On average, OECD countries spend around 2.35 per cent of GDP on family benefits, with levels ranging from 0.5 to 3.5 per cent1. This includes one-off cash transfers and regular payments around the time of childbirth to support families.
Countries including Australia, Poland, Spain, South Korea, Switzerland, and UK have introduced one off ‘baby bonus’ payments to alleviate the financial pressures of having a child and improve equity in early life. Examples of one-off payments include: Australian Baby Bonus (2004-14; A$3000); Spain Maternity Bonus (2007-10; €2500); South Korea Baby Bonus (2000-15; US$680-2350); Swiss Baby Bonus (1969-2017; CHF 1000-1500); US NICU Financial Support programme (2017-2018; $600). Some one-off cash transfers are conditional on health behaviours or care giving, like the UK HiP (2009-2011; £190). These include: Poland Baby Bonus (2006-; €262); the US Healthy Pregnancy Program (1998-2001; $100).
Examples of regular payments include the Manitoba Healthy Baby Prenatal Benefit Program in Canada (2001-; C$10-$81.41 monthly from 14 weeks pregnancy until birth); Rx Kids in Flint, US (2024-; $1500 one-off payment mid pregnancy plus $500 monthly from birth to age 1); US Baby's First Years (2018-; $20 or $333 monthly payments from birth to age 6). Key features of each policy are summarised in Table A3.
Section 3: One off cash transfers in first 1000 days and child health outcomes
3.1 Summary of key findings
Targeted one-off transfers are consistently more effective than universal bonuses, with benefits concentrated among disadvantaged families and largely null average effects from universal schemes.
Conditional transfers linked to prenatal care increase service use, but unconditional bonuses alone may have limited impact.
Timing matters more than size, with modest payments during pregnancy improving birth outcomes, while large postnatal transfers show little population-level impact.
3.1.1 Universal and targeted cash transfers
Across 13 studies, targeted one-off cash transfers are better than universal ones at improving early-life health. In studies of targeted policies, over 60 per cent of outcomes were positive (Figure 2). Universal bonuses (e.g. Australia, Spain) tend to produce null average effects on child health and development, even when generous. In contrast, effects for targeted policies are larger, more consistent, and more robust among disadvantaged groups (low-income families, younger mothers, single mothers, low-education households), particularly for birth outcomes and early health service use.
Percentage of early years outcomes showing positive and null effects.
3.1.2 Unconditional and conditional cash transfers
Conditionality matters primarily when policies are directly aimed at improving health behaviours. More than half of early years outcomes were positive in the studies of conditional policies (Figure 3). Conditional programmes tied to prenatal care engagement (e.g. US Healthy Pregnancy Program, Poland Baby Bonus) show improvements in service uptake and downstream reductions in neonatal morbidity, even with/without strong effects on birthweight. Cash transfers conditional on administrative milestones (e.g. attending a single antenatal visit, as with UK HiP Grant) show mixed or null impacts on birth outcomes. This suggests that the cash itself, rather than the condition, often drives effects unless the condition meaningfully changes behaviour.
Percentage of early years outcomes showing positive or null effects.
3.1.2 Value of cash transfers
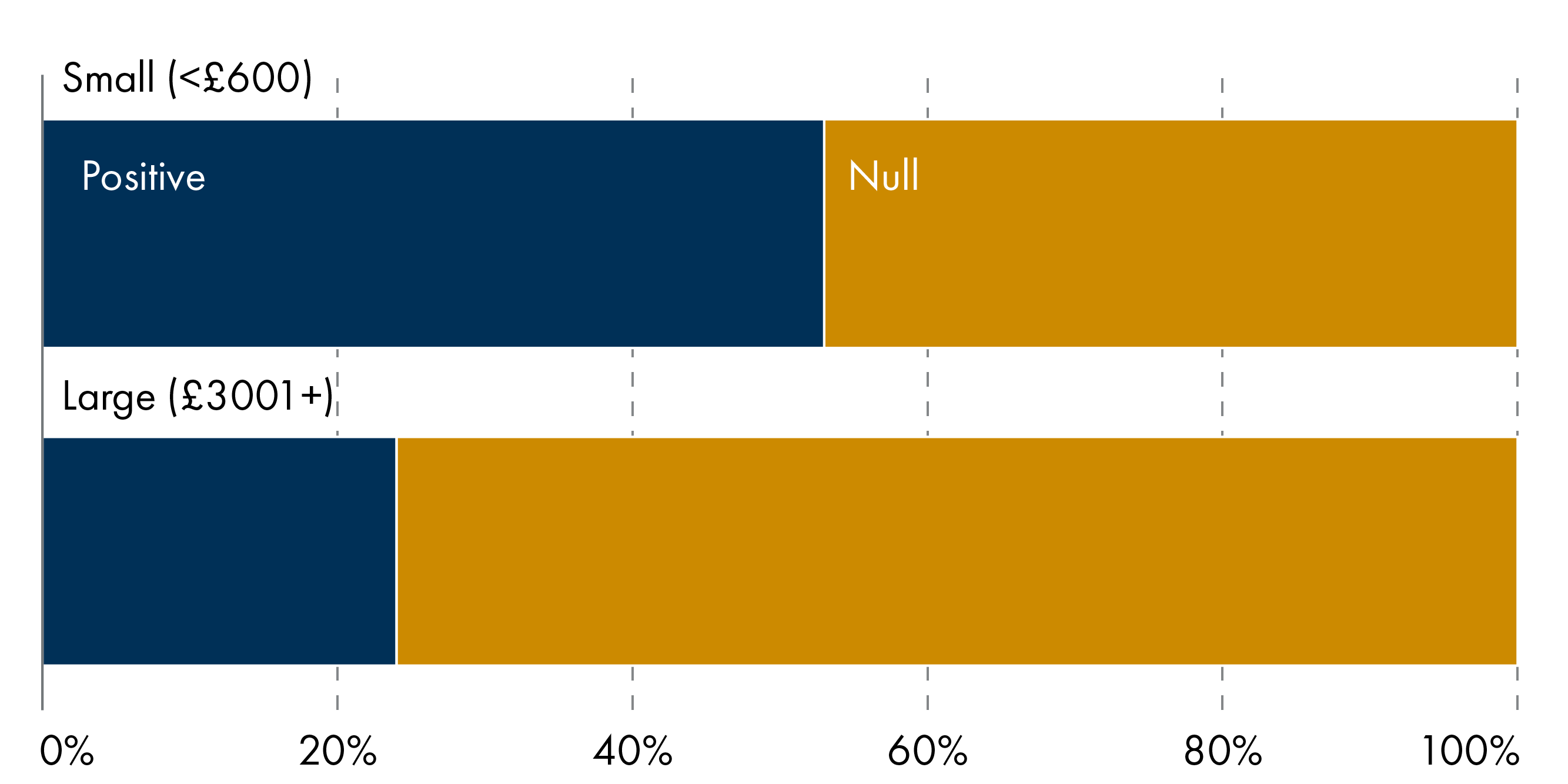
There is no simple dose–response relationship between transfer size and outcomes. Small (<£600) to medium (£1000-£3000) size payments (e.g. HiP Grant; Poland Baby Bonus; Swiss Baby Bonus) can generate detectable improvements in birth outcomes, while large (£3001+) transfers (e.g. Spain Baby Bonus) often do not at the population level (Figure 4). Timing and context appear to matter more than size: transfers paid during pregnancy are more likely to affect fetal health, while postnatal one-off payments show little evidence of improving later child health or development.
Percentage of early years outcomes by payment size (grant amounts converted to GBP and indexed to 2026 values)
3.2 Evidence on one off cash transfers in first 1000 days by outcome
3.2.1 Summary of key outcomes
▲ Cash transfers paid during pregnancy improve birth outcomes, with reductions in low birthweight and prematurity concentrated among disadvantaged mothers and preterm infants; postnatal one-off bonuses show little effect, and negative average effects reflect changes in who gives birth (e.g. more births to disadvantaged mothers), not harm caused by the payment.
▲ One-off payments substantially reduce infant emergency care and hospitalisations in the short term, particularly among disadvantaged families, but these service-use effects are time-limited and do not automatically translate into improved birth outcomes.
<> ▲ There is little or no evidence that one-off cash transfers produce sustained improvements in child health or development beyond infancy, with large studies reporting precise null effects across cognition, physical and socio-emotional outcomes. There are, however, notable small subgroup gains.
Number of positive and null outcomes by type of early years outcome and study quality.
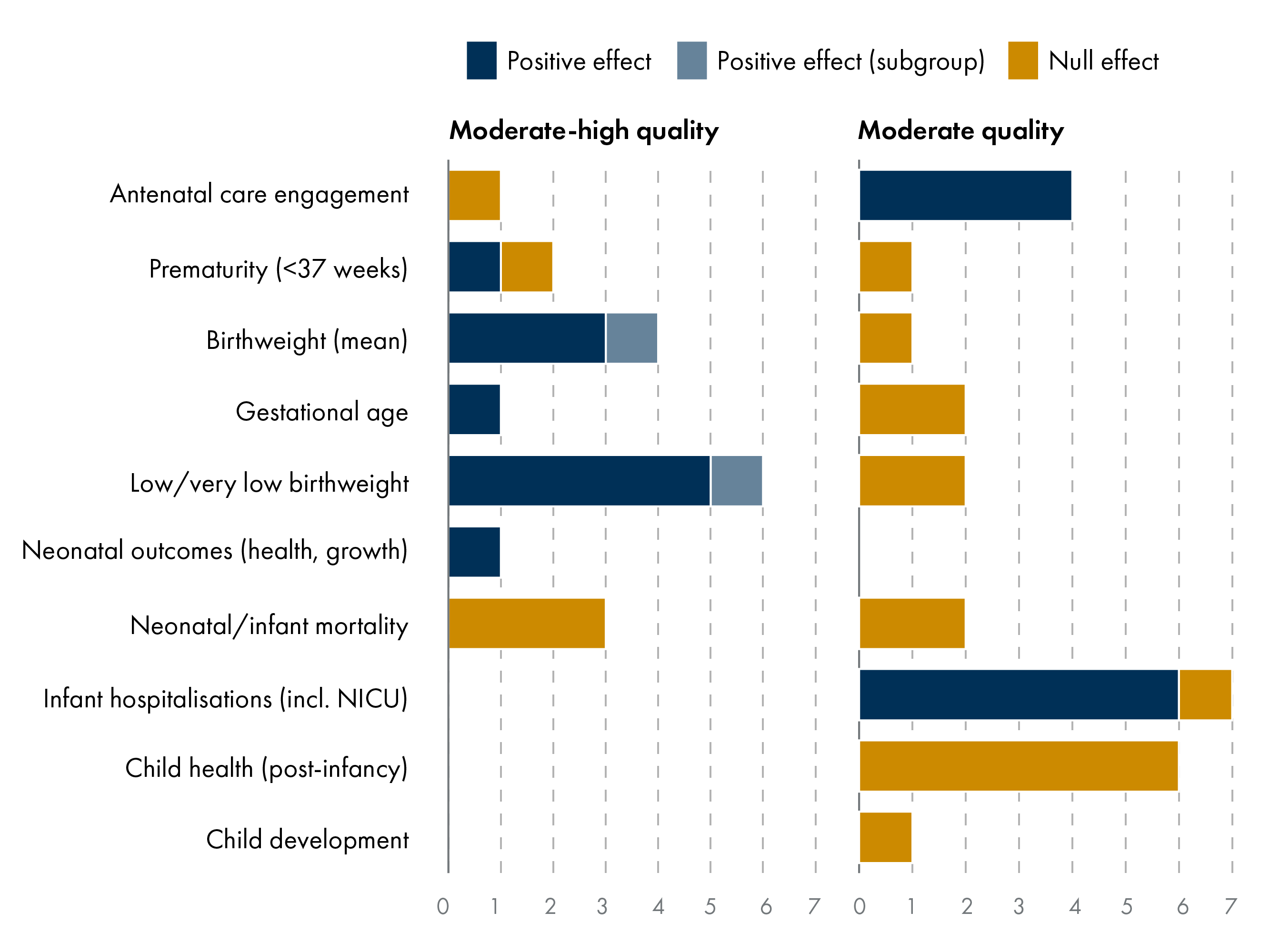
Of the 13 studies reviewed, the majority (77% of studies, 80% of outcomes) were rated as moderate or moderate-to-high quality. As shown in Figure 5, the positive impact of one-off cash transfers is most strongly observed in birth outcomes including antenatal engagement, birthweight, and low birthweight. There are also short-term improvements in infant hospitalisations. All outcomes that measured child health and development show no effect and are from moderate or low-moderate quality studies.
The highest-quality studies provide robust evidence of causal impacts on birth outcomes and healthcare utilisation. The geographically diverse studies were methodologically strong, using quasi-experimental designs (e.g. difference-in-difference and regression discontinuity) and large administrative datasets.
The following sections examine the three different outcome groups in more depth: birth outcomes, child health and development, and health service use. The symbols indicate ▲positive and <> null findings.
3.2.2. Birth outcomes
Key findings
▲ Birth outcomes improve when cash is paid during pregnancy, likely by supporting maternal health and reducing early delivery.
▲ Strong effects are observed among disadvantaged mothers and preterm infants, indicating families with more challenges or fewer resources likely benefit the most.
<> Postnatal one-off bonuses show little or no effect, with negative averages reflecting changes in birth timing rather than harm.
Evidence from several large, moderate-high rated studies indicates that one-off cash transfers during pregnancy can improve birth outcomes, particularly among subgroups. For example, in the UK, Reader (2023)1 reports that the universal £190 Health in Pregnancy Grant increased mean birthweight by 8–12 g at the population level. The effects are small for individual babies but meaningful across the population. The policy also reduced low birthweight by 0.2–0.4 percentage points (3–6%) and prematurity by 0.6–0.8 percentage points (9–11%), with substantially larger effects for younger and socio-economically disadvantaged mothers (birthweight increases of ~25 g and a 17% reduction in very low birthweight). These effects appeared to operate primarily through longer gestation rather than changes in antenatal care use, suggesting that additional income late in pregnancy helped reduce early delivery.
Similarly, in Spain, González et al. (2022)2 provide evidence that a one-off €2,500 baby bonus substantially improved fetal health for subsequent children, with effects concentrated at the lower end of the birthweight distribution. Gains were most notable for disadvantaged preterm infants including 100–228 g (5–12%) increases in birthweight and 49–83 per cent relative reduction in very low birthweight. So, while the bonus did not raise average birthweight, it did improve outcomes at the lower tail of the distribution, reducing very low birthweight and shifting vulnerable infants into healthier weight ranges. This was plausibly linked to improved maternal health and behaviours rather than changes in pregnancy timing.
Multiple large studies of one-off payments in Australia, Switzerland, and UK provide robust null evidence for several birth outcomes. In some instances, there are negative impacts reported but these largely reflect changes in birth timing rather than harm. For example, Kim (2024)3suggests that negative average effects are due to a selection effect, namely changes in who is giving birth and shorter pregnancies. And once gestational age is considered, cash transfers may help fetal growth in low-income families. This highlights the difference between overall population averages and positive effects for disadvantaged groups.
3.2.3 Child health and development
Key findings
<> No consistent effects reported on child health or development beyond infancy.
<> Postnatal one-off cash may be insufficient to change long-term trajectories, with no impact on cognition, physical health, or socio-emotional outcomes.
▲ Limited subgroup gains are evidenced for disadvantaged groups e.g., children of less-educated parents.
Across contexts, there is little evidence that one-off cash transfers lead to sustained improvements in child health or developmental outcomes beyond infancy. Using linked administrative data, Borrà et al. (2024)1 find no evidence that the one-off Spain Baby Bonus (€2,500) affected child health or educational outcomes in either the short or medium term. This moderate rated study reports null effects on birth outcomes, child anthropometrics, primary care use, hospitalisations (ages 0–8), and primary school test scores. Estimates are sufficiently precise to rule out even modest health improvements, including reductions in overweight/obesity or health care use. No effects are observed for disadvantaged households. The authors suggest that a generous, unconditional cash transfer paid after birth is unlikely to meaningfully influence child health or development.
Two low-moderate quality studies of the one-off Australian Baby Bonus (A$3000) similarly find no evidence that the policy improved average child health or educational outcomes. Gaitz & Schurer (2017)2 found no aggregate effects on children's cognitive, socio-emotional, or physical health outcomes through age 12-13. Observed effects were small, often statistically insignificant, and in some cases reflected parental perceptions. While Deutscher and Breunig (2018)3 found no evidence of improvements in child health or educational outcomes at the population level, modest gains were observed in disadvantaged subgroups. Improvement (~0.04 SD) in NAPLAN reading and numeracy scores at ages 8–9 was reported among children of less-educated parents.
3.2.4 Health service use
Key findings
▲ One off transfers lead to substantial short-term reductions in infant emergency care and hospitalisations, particularly for respiratory conditions, likely by reducing risk exposure and supporting preventive care.
▲ Effects are strongest among disadvantaged families, reflecting higher baseline barriers.
<> Service-use effects are time-limited and do not automatically translate into improved birth outcomes.
A notable impact of one-off cash transfers is observed in infant health service use. Robust, moderate quality evidence comes from large administrative datasets in Australia. Exploiting the unanticipated introduction of the Australian Baby Bonus (A$3000), de Gendre (2021)1 found a significant reduction in urgent, acute, and preventable hospital presentations in the first two years of life, particularly for respiratory conditions such as bronchiolitis. Treated children were less likely to require emergency department admission or inpatient services, while elective and planned care increased in year two, suggesting a shift from reactive to preventive health care. No evidence was found of increased accidents or the need for longer-term diagnostic service use. These gains did not persist beyond infancy. Complementing this, Rosenthal et al. (2009)2 show that a conditional prenatal care incentive programme in the US increased adherence to recommended care to 76 per cent and reduced the odds of NICU admission by 55 per cent (OR 0.45; 95% CI 0.23–0.88). Despite these positive effects, there was no statistically significant effect on birth outcomes, including birthweight, prematurity, or neonatal mortality.
One-off payments are effective at influencing engagement and behaviour during pregnancy but do not necessarily translate into measurable improvement in birth outcomes. Two evaluations of the UK HiP Grant find earlier antenatal booking and increased engagement, but no corresponding reductions in adverse birth outcomes. Leyland et al. (2017)3 find clear improvements in antenatal engagement following the introduction of the HiP Grant, with mean gestational age at booking decreasing by 0.35 weeks (95% CI 0.29 to 0.41) and the odds of booking before 25 weeks increasing by 10 per cent (OR 1.10; 95% CI 1.02 to 1.18), equivalent to around 600 additional women per year accessing antenatal care earlier. Apparent reductions in neonatal mortality were not robust across specifications and likely reflect broader improvements in neonatal care rather than a causal effect of the grant. Adams et al (2017)4 also found meaningful medium-term improvements in antenatal care engagement, including earlier booking and higher proportions of women attending by key gestational thresholds, effects that reversed following policy withdrawal. The policy was not associated with changes in infant size at birth, including the risk of being small for gestational age. The authors note that the magnitude of the improvement in booking timing (approximately 4.8 days at 21 months) may have been too small to plausibly influence fetal growth.
Section 4: Regular cash transfers in first 1000 days and child health outcomes
4.1 Summary of key findings
Small regular cash transfers can result in positive child health outcomes, whereas studies of large total transfers mostly report null findings.
Regular cash transfers produce the most significant improvements in birth and health outcomes when targeted at vulnerable groups (such as low-income or Indigenous mothers).
Regular payments for low-income mothers can be successful in narrowing socio-economic gaps in areas like preterm births and low birthweight.
4.1.1 Value of cash transfers
All programmes providing regular cash transfers in the first 1000 days were unconditional and either universal or targeted to low-income populations. For example, the Rx Kids program in Flint (US) offered universal payments, whereas the Manitoba Healthy Baby Prenatal Benefit (Canada) and US Baby's First Years focused on low-income mothers, but all three were unconditional. Within this sample, therefore, it is not possible to assess how conditionality affects outcomes.
There is sufficient variation to explore whether the magnitude of cash support (i.e. total payments over time) is associated with differences in early years outcomes. All three policies provide monthly payments to mothers, except for Rx Kids that includes an additional one-off mid-pregnancy payment. Payment duration ranges from one year (Rx Kids, Manitoba Healthy Baby Prenatal Benefit Program) to six years (US Baby's First Years).
Smaller cash transfers (totalling <£600 when summed across multiple payments) were associated with 24 positive outcomes whilst 21 were null, indicating mixed results at low amounts (Figure 6). Large total transfers (£3001+) were positive for six outcomes and 19 outcomes were null. While high-value transfers may be impactful, detectable benefits may plateau or be concentrated in specific outcomes or subgroups.
Percentage of early years outcomes by payment size (grant amounts converted to GBP and indexed to 2026 values)
4.1.2 Targeting and equity
Variation in outcomes appears closely linked to population targeting and baseline inequities. The Manitoba Healthy Baby Prenatal Benefit consistently showed larger effects among broader low-income populations. Brownell et al. (2010, 2016)12 report reductions in preterm birth and low birthweight among low-income women. Brownell et al. (2018)3further demonstrated that the Manitoba Prenatal Benefit narrowed socio-economic inequities, reducing the absolute gap in low birthweight by almost 2 percentage points and by 29 per cent in relative terms. Similarly, analyses by Enns et al. (2021)4 and Struck et al. (2021)5 found that First Nations women experienced improvements in birth outcomes and early childhood immunisation, whereas Métis women had gains in birth outcomes but limited developmental effects. In contrast, the Rx Kids program6 improved prenatal care utilisation across the population, but as a near-universal program, it provides little insight into differential effects by socio-economic subgroups. Overall, cash transfers appear to produce the largest detectable improvements in populations with higher vulnerability, underscoring the importance of policy targeting.
4.2 Evidence on regular cash transfers in first 1000 days by outcome
4.2.1 Summary of key outcomes
▲ Regular cash transfers during pregnancy increase the use of prenatal care services, including earlier initiation and more adequate prenatal care (composite measure of care initiation, number of visits, and pregnancy duration) but impacts on postnatal health service use, immunisations, and hospitalisations are mixed.
▲ Consistent financial support in pregnancy is associated with lower risks of preterm birth and low birthweight in low-income populations.
<> ▲ Studies find little or no sustained improvements in child health or development beyond infancy, with null effects on cognition, socio-emotional skills, and physical health up to preschool age. Positive effects are reported for disadvantaged groups.
Number of positive and null effects by type of early years outcome.
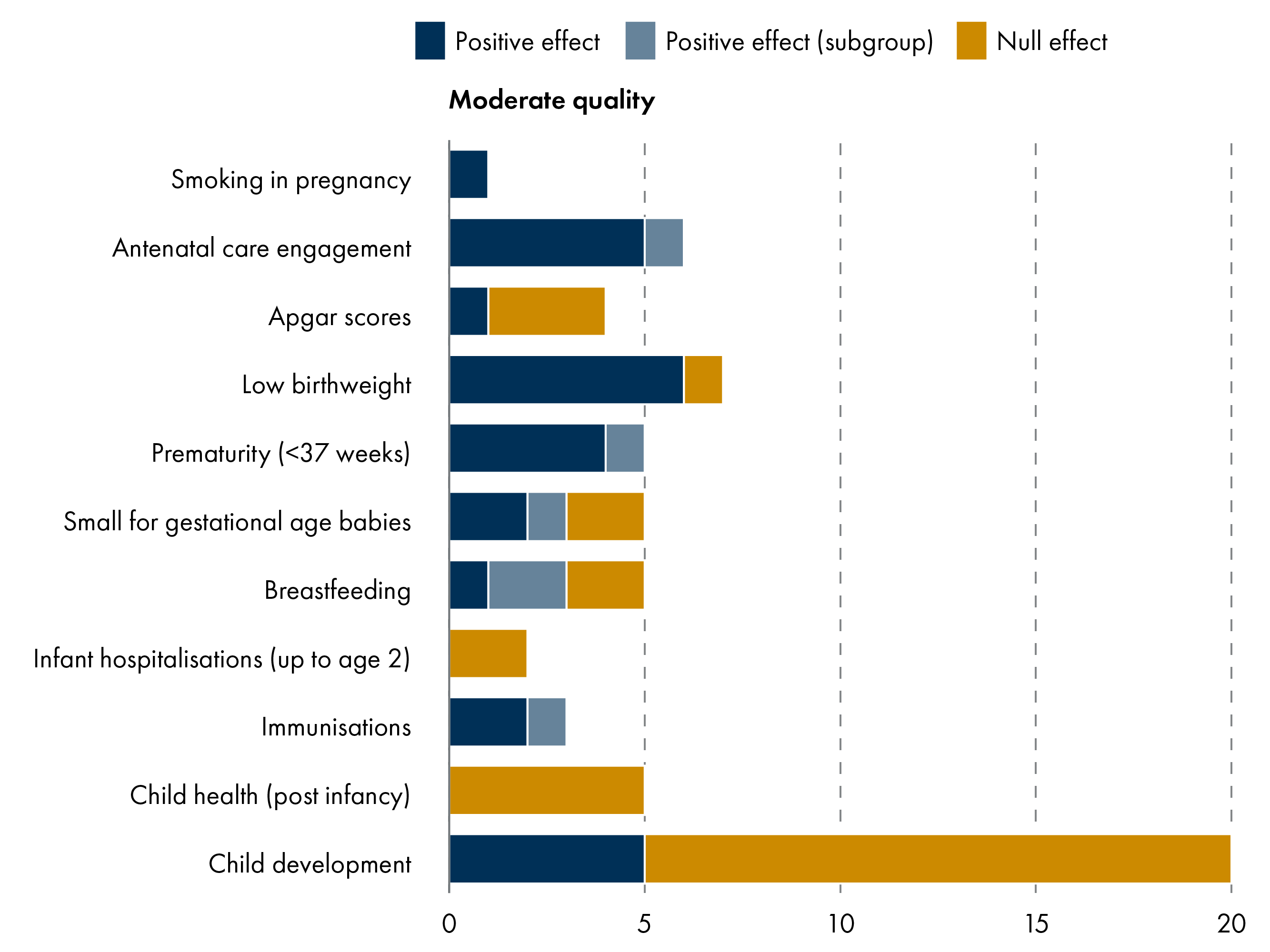
As observed in Figure 7, there are several positive impacts of regular cash transfers in the prenatal and postnatal stage including antenatal care, prematurity and low birthweight. Some studies find positive outcomes for child development measures, but the majority are null.
The 14 studies reviewed were all rated as moderate quality. Study design includes a randomised control trial (RCT) and cohort studies. While the three Canadian studies123 use overlapping administrative datasets, each examine distinct cohorts, time periods and outcomes. Similarly, the US Baby's First Years papers report different outcomes and findings from multiple time points.
The following sections examine the three different outcome groups in more depth: birth outcomes and infant health, child health and development, and health service use. The symbols indicate ▲positive and <> null findings.
4.2.2. Birth outcomes and infant health
Key findings
▲ Regular prenatal cash transfers were associated with lower risks of preterm birth and low birthweight in low-income populations.
▲ Breastfeeding initiation increased modestly when cash transfers were combined with community support programmes.
<> Inconsistent evidence on birthweight, while studies report no impact on infant health or hospital readmissions.
Findings from Manitoba (Canada) consistently show that unconditional prenatal cash transfers improve birth outcomes among low-income mothers. Brownell et al. (2016)1 found that recipients of the Healthy Baby Prenatal Benefit were 17.5 per cent less likely to experience preterm birth and 21 per cent less likely to have a low birthweight infant (RR 0.76 and 0.71, respectively), while breastfeeding initiation increased slightly (RR 1.06). Earlier work on the Manitoba policy2 found that breastfeeding initiation increased significantly when the Prenatal Benefit was combined with participation in Community Support Programs. So cash transfers may need to be delivered alongside additional support to improve some outcomes.
Analyses among First Nations and Métis populations showed mixed findings: Enns et al. (2021)3 reported 26 per cent lower risk of low birthweight and 23 per cent lower preterm birth among First Nations women, along with improved immunisation and language outcomes. Likewise, Struck et al. (2021)4 found that birth outcomes improved among Métis women, but developmental effects were not observed.
Evidence across the studies above was inconsistent regarding birthweight (small or large for gestational age babies) and payments showed no significant impact on Apgar scores, neonatal admissions, or infant hospitalisations.
4.2.3 Child health and development
Key findings
▲ Modest improvements in early neurodevelopmental markers were observed at age 1 following monthly unconditional cash transfers.
<> Effects on cognitive, language, socio-emotional development, or pre-literacy skills up to age 4 were generally null.
<> Regular prenatal cash transfers show limited effects on longer-term child development.
The US Baby's First Years trial provides detailed insight into child health and early development following regular monthly unconditional cash transfers of $333 USD per month (compared to $20). Troller-Renfree et al. (2022)1 found that a high-cash transfer (~20% income increase) was associated with higher mid- to high-frequency EEG activity at age 1 (effect sizes 0.17–0.26), indicative of potential cognitive and language benefits.
Follow-up studies of the US Baby's First Years families at years 3 and 4 have documented mostly null outcomes. This includes language, executive function, socio-emotional outcomes, and brain activity (except a modest increase in relative alpha power at age 4)234. Sperber et al. (2023)5 report no significant differences in child health, sleep, or healthcare utilisation between high- and low-cash groups, except for higher fresh produce consumption at age 2. While poverty reduction in infancy may influence early neurodevelopmental markers, regular cash transfers alone may not be sufficient to drive measurable gains in cognitive or socio-emotional outcomes by preschool age.
4.2.4 Health service use
Key findings
▲ Regular cash transfers increase utilisation of prenatal care services leading to earlier initiation and more adequate care.
▲ Improvements are reported for prenatal care and immunisations for Indigenous and low-income mothers.
<> Evidence on infant and postnatal health is limited with broader health outcomes and hospitalisation rates often showing no change.
Cash transfer programmes consistently improve engagement with prenatal health services. The Rx Kids program increased adequate prenatal care (incl. care initiation, no of visits and pregnancy duration) by 9.1 percentage points and first-trimester initiation by 5.6 percentage points (95% CI 2.5–8.7), highlighting strong uptake in a universal policy1. In Manitoba, Brownell et al. (2010, 2016)23 found improvements in prenatal care, particularly among women receiving income assistance. In both studies, infant health measures were either not assessed or were largely unaffected.
Postnatal health service utilisation shows a mixed pattern. For instance, immunisation completion improved in First Nations and Métis populations45, whereas broader infant hospital use did not show consistent changes. While cash transfers can enhance service engagement during pregnancy, their effects on downstream health service utilisation for infants and young children may be limited.
Section 5: Cash transfers and child health inequalities
5.1 Summary of studies reporting sub-group effects
Key findings
▲ Universal, one-off payments improve child health outcomes among sub-groups such as low-income or younger mothers.
▲ Targeted, regular payments improve the child health outcomes of disadvantaged families.
X Few studies formally considered effects on child health inequalities although beneficial findings among disadvantaged groups imply potential to modestly reduce inequalities at the population level.
Cash transfers during pregnancy and early childhood may potentially reduce health inequalities. Several studies report positive health outcomes for children in vulnerable households, but more high-quality evidence is needed to fully understand the impact on health inequalities in young children.
Where one-off pregnancy payments show health benefits, these are most often concentrated among younger, lower-income, or otherwise disadvantaged mothers. Studies show that one-off cash payments can improve birth outcomes1, increase access to antenatal care2, reduce infant hospitalisations3 and lead to improvements in reading/numeracy4 among disadvantaged families.
There is some evidence that regular, targeted payments can reduce socio-economic inequalities in birth outcomes. Brownell et al (2018)5 found that regular payments were associated with narrowing the disparity between low‑ and higher‑income women's birth outcomes including low birthweight, preterm birth and breastfeeding initiation. The reduction in inequities reflected an improvement for disadvantaged women and a relative closing of the gap with better‑off families, suggesting a movement toward greater population‑level equity in birth outcomes.
Despite these findings, however, nearly half of studies did not report on whether cash transfers reduce child health inequalities. For example, evaluations of universal, one-off policies (Australian Baby Bonus6; Swiss Baby Bonus7) did not assess differential impacts, highlighting an evidence gap in understanding whether average health gains translate into meaningful reductions in socio-economic disparities.
Section 6: Key findings
This review provides evidence to justify continued policy commitment to supporting families during the critical first 1,000 days of life. Key findings are:
Child-focused cash support is an evidence-based upstream intervention that improves early child well-being and strengthens developmental foundations – even with modest investment amounts.
Well-designed cash transfers in pregnancy and early childhood improve birth outcomes and support early development – with no evidence of harm and potential to reduce inequalities.
The most effective early-years income supports are unconditional, recurring, and delivered early in pregnancy to low-income families; these programmes consistently improve birth outcomes and early child development, while one-off bonuses have modest effects.
6.1 Summary of outcomes
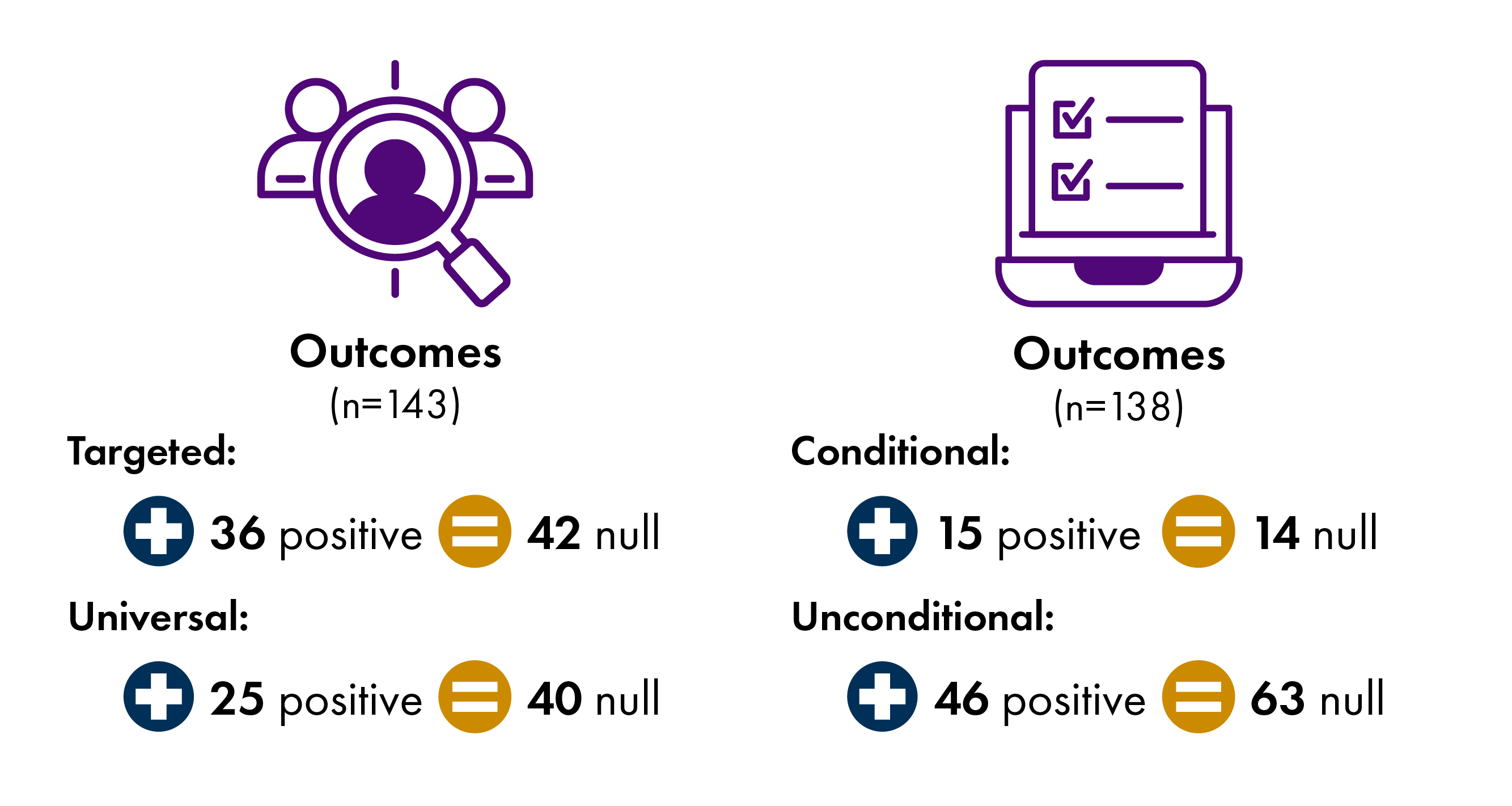
Each of the 27 studies in this review looked at numerous outcomes. Overall there was more positive evidence for targeted rather than universal payments (36 vs 25 outcomes), and more positive evidence for unconditional rather than conditional payments (46 vs 15 outcomes) (Figure 8). While no studies found negative impacts, a substantial number did find null effects. Regular, targeted support for low-income families with young children is well supported by the existing research.
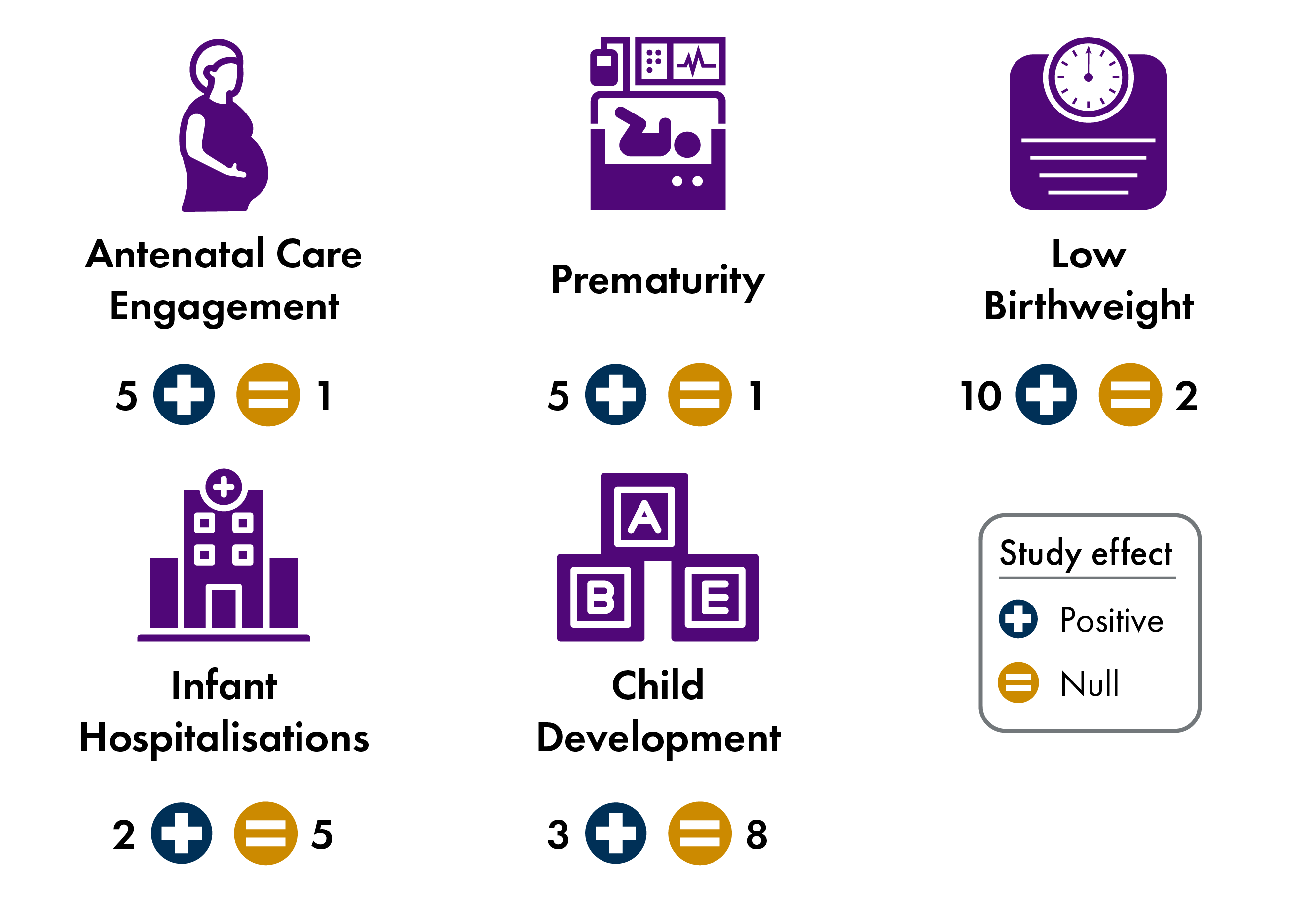
Figure 9 summarises results by type of early years outcome. Across the 27 studies, ten found positive effects on low birthweight, five found greater engagement in antenatal care and five found reductions in premature births. Both one-off and regular cash transfers improve prenatal care and birth outcomes. For infant hospitalisations, only one-off cash transfers showed some improvements. Both one-off and regular cash payments report mostly null effects for child health outcomes, with three studies linked to positive child development outcomes.
6.2 Key insights
To conclude, this section identifies the key takeaways from the evidence review and reflects on how this relates to existing causal pathways.
1. Timing matters: the evidence consistently highlights the prenatal period as a critical window for intervention.
Birth outcomes: prenatal cash transfers are associated with significant reductions in low birthweight and preterm births; birth outcomes that influence long-term developmental pathways, cognitive function, and adult chronic disease risk.
Prenatal care: cash transfers during pregnancy significantly increase engagement with antenatal services, particularly encouraging earlier initiation of care within the first trimester.
Evidence suggests that postnatal transfers have a more limited impact on overall childhood health and development compared to support provided during the critical prenatal window.
2. Payment structure: the evidence shows a preference for regular payments over one-time bonuses.
One-off transfers were found to have a modest effect on long-term childhood health outcomes or development. Such payments are often treated like ‘windfalls’ rather than a reliable increase in household income.
Predictability: regular, predictable payments are more likely to enable parents to make sustained investments in their children's development.
3. Targeting and conditionality: positive impacts on child health are typically highest when directed at the most disadvantaged families.
Targeting: targeted schemes show more consistent positive results than universal, one-off payments and demonstrate the most potential for closing the gap in child health inequalities.
Conditionality: the evidence for conditionality is limited to payments linked to health care engagement, particularly during the antenatal period.
4. Generosity and inflation adjustment: while lower payment amounts can be effective, if inflation erodes its value too much it can cease to have an impact.
Diminishing returns: The impact of Manitoba’s Healthy Baby Prenatal Benefit diminished over 20 years. Eroded by inflation, the benefit failed to improve birth or developmental outcomes by 2019.
5. Mechanisms and causal pathways: the effectiveness of transfers is believed to work through several specific channels.
Investment model: families use one off payments to purchase essential baby items and improve the home environment. Regular transfers allow mothers to invest in maternal well-being and prenatal care, providing a foundation for fetal development.
Parental stress model: direct cash helps mitigate maternal stress during pregnancy, which is a known driver of health inequalities and adverse birth outcomes.
Behavioural change: cash transfers can encourage sustained engagement with maternity and postnatal health services, which may contribute to improved outcomes at birth and during infancy.
Appendix
A1 Research approach
A1.1 Evidence search
International evidence was identified through a multi-stage search and screening process. First, relevant studies were drawn from 54 child health papers identified by a recent scoping review 1. Second, this list was cross-checked against all references in 11 additional systematic reviews 23456789101112 and a policy mapping review13. Third, the search was supplemented by keyword searches of PubMed and Google Scholar. In total, these searches identified 119 papers.
Quantitative evaluations of cash transfers in high income countries were included where: the study population was infants or children up to age five; cash transfers were delivered within the first 1,000 days; the transfers were child-focused and intended to benefit children; and outcomes related to child health or health inequalities. Titles and abstracts were screened, resulting in 27 included papers. Family income supplements (such as dividends or lottery winnings), transfers conditional on parental employment, general social security income payments or child benefits, and in-kind transfers were excluded (71 papers). A further 21 papers were excluded because they did not report child health outcomes.
The final evidence base comprises 27 papers: 13 evaluating one-off cash transfers and 14 examining regular payments, delivered during the first 1000 days. A total of 144 early years outcomes were recorded across the studies.
A1.2 Outcome direction coding
Effects are coded where estimates were statistically distinguishable from zero. Findings observed only in subgroup analyses, alternative bandwidths, or sensitivity specifications are noted and described narratively. Direction of effect was coded to reflect desirability, with upward arrows indicating beneficial effects (▲), downward arrows indicating harmful effects (▼), and neutral symbols indicating a null effect (<>).
A1.3 Quality ratings
To appraise each study, a quality rating was assigned. This qualitative judgement reflects strength of study design, quality and completeness of the data, analytical methods (informed by Joanne Briggs Institute (JBI) appraisal checklists141516 used to assess the reliability, applicability, and methodological rigour of published studies) and consistency of results. A sample of the quality ratings was double-checked by two independent reviewers.
Moderate-High: Strong confidence that the study results reflect real effects in the population, the study is well-designed, uses reliable data, large sample, and outcomes are clear, meaningful, and robust across analyses.
Moderate: Reasonably confident in the study results, but some uncertainty remains due to factors such as small sample sizes, short follow-up, limited outcome measures, or reliance on indirect indicators.
Low-Moderate: Study design is appropriate, but confidence is limited because effects are short-term, mostly null, or outcomes are based on parent reporting or mechanically driven (e.g. timing effects rather than behavioural change).
Table A1: Summary of findings - one off cash transfers in first 1000 days (n=13)
| Policy | Study | Outcomes and direction of effect | Quality rating |
|---|---|---|---|
| Australian Baby Bonus | de Gendre et al (2021)1 | ▲ preventable hospitalisations (year 1–2)▲ urgent/acute hospital presentations▲ ED presentations requiring admission▲ respiratory presentations (bronchiolitis)▲ elective/planned care (year 2)<> accidents/injuries<> subsequent diagnostics (up to age 5) | Moderate |
| Australian Baby Bonus | Deutscher & Breunig (2018)2 | <> gestation length (▲ due to birth timing)<> birthweight (▲ mechanically via delayed delivery)<> infant health and development (not directly measured; pathways discussed only)<> reading and numeracy at age 8-9 (▲for disadvantaged children) | Low-moderate |
| Australian Baby Bonus | Gaitz and Schurer (2017)3 | <> physical health outcomes<> chronic health conditions<> BMI/weight indicators<> cognitive skills<> socio-emotional skills<> behavioural problems | Low-moderate |
| Poland Baby Bonus | Cygan-Rehm & Karbownik (2022)4 | ▲ neonatal health index▲ birthweight▲ low birthweight▲ fetal deaths<> gestational age | Moderate-high |
| South Korea Baby Bonus | Kim (2024)5 | ▼ gestational age (2nd & 3rd births, reflects timing/selection)▼ birthweight (driven by preterm birth/selection)▼ preterm birth (2nd & 3rd births)<> early life mortality | Moderate-high |
| Spain Maternity Bonus | Borrà et al (2024)6 | <> height/weight (0-4)<> BMI (0-4)<> overweight/obesity (0-4)<> primary care visits (0-4)<> primary care diagnoses/health problems (0-7)<> primary care referrals (0-7)<> hospitalisations (respiratory, infections, injuries, perinatal and mental health) (0-8)<> school performance (test scores in primary school, grade repetition) | Moderate |
| Spain Maternity Bonus | Gonzalez and Trommlerová (2022)7 | ▲ very low birthweight (<1500g)▲ birthweight distributional (shift from <1500/2000g into healthier ranges)<> low birthweight (▲poor/ unmarried mothers, preterm births)<> mean birthweight (▲ preterm births, esp. poor families)<> birth spacing<> gestational age<> prematurity<> early neonatal mortality | Moderate-high |
| Swiss Baby Bonus | Chuard & Chuard-Keller (2021)8 | ▲ low birthweight (effect at cut-off)▲ birthweight (attenuates over time, robust at intro)<> infant death<> stillbirths | Moderate-high |
| UK Health in Pregnancy Grant (HiP), England & Wales | Adams et al (2018)9 | ▲ antenatal care outcomes (mean gestational age at booking, midwife booking)<> small for gestational age babies | Moderate |
| UK Health in Pregnancy Grant (HiP), Scotland | Leyland et al (2017)10 | ▲ antenatal care (earlier booking)▲ antenatal care (odds of booking)<> smoking during pregnancy<> Apgar scores<> mean birthweighti<> low/very low birthweight<> small for gestational babies<> preterm birth<> stillbirths<> neonatal mortalityii<> infant mortality<> emergency caesarean section (inconsistent / unclear attribution) | Moderate |
| UK Health in Pregnancy Grant (HiP), England and Wales | Reader (2023) 11 | ▲ low birthweight (<2500g)▲ very low birthweight (<1500g)▲ birthweight▲ prematurity (<37 weeks)▲ gestation age<> antenatal care timing (first visit) | Moderate-high |
| US Healthy Pregnancy Program | Rosenthal et al (2009)12 | ▲ prenatal care initiation and attendance▲ NICU admission▲ infant care costs (first year)<> low birthweight | Moderate |
| US NICU Financial Support | Andrews et al (2020)13 | ▲ skin-to-skin contact▲ NICU visitation/parental presence▲ breastfeeding (milk provision)<> neonatal length of stay<> neonatal growth | Low-Moderate |
Table A2: Summary of findings - regular cash transfers in first 1000 days (n=14)
| Policy | Study | Outcomes and direction of effect | Quality rating |
|---|---|---|---|
| Rx Kids, USi | Hanna et al (2025)1 | ▲ adequate prenatal care (Kessner Indexii)▲ no prenatal care▲ antenatal care (number of visits)▲ antenatal care timing (increased first trimester initiation) | Moderate |
| Manitoba Healthy Baby Prenatal Benefit Program, Canada | Brownell et al (2010)iii2 | ▲ low birthweight▲ preterm birth▲ prenatal care engagement (earlier, consistent care)▲ breastfeeding initiation (only + Community Support Program)<> adequate prenatal care (▲ pop 2 only)<> small for gestational age babies (▲ pop 2 only)<> large for gestational age babies (▼ pop 2 only)<> congenital anomalies<> hospitalisations (incl. injury hospitalisations)<> 2-year immunisation (▲ pop 2 only) | Moderate |
| Manitoba Healthy Baby Prenatal Benefit Program, Canada | Brownell et al (2016)3 | ▲ low birthweight▲ preterm birth▲ breastfeeding initiation▲ hospital length of stay (vaginal births)▲ small for gestational age babiesiv<>/▲ large for gestational age babies (increase, interpretation uncertain)<> Apgar scores<> hospital length of stay (caesarean births)<> neonatal readmission (within 28 days) | Moderate |
| Manitoba Healthy Baby Prenatal Benefit Program, Canada | Brownell et al (2018)4 | ▲ low birthweight▲ preterm birth (women in urban areas only)▲ breastfeeding initiation (women in rural areas only) | Moderate |
| Manitoba Healthy Baby Prenatal Benefit Program, Canada | Enns et al (2021)5 | ▲ low birthweight▲ preterm birth▲ complete immunizations at age 1 and 2▲language and cognitive development▲ communication skills and general knowledge<> small for gestational age babies<> large for gestational age babies<> Apgar scores<> neonatal readmission (28 days)<> hospital length of hospital stay<> hospital readmission in first 2 years<> physical health and well-being<> social competence<> emotional maturity | Moderate |
| Manitoba Healthy Baby Prenatal Benefit Program, Canada | Enns et al (2025)6 | ▲ low birthweight▲ preterm birth▲ small for gestational age babies▼ large for gestational age babies▲ breastfeeding initiation<> all early period only – attenuates over time▲ early childhood development (language/cognitive)<> early cohorts only | Moderate |
| Manitoba Healthy Baby Prenatal Benefit Program, Canada | Struck et al (2021)7 | ▲ low birthweight▲ preterm birth▲ vaccination at age 1 and 2▼ large for gestational age babies (higher risk)▼ neonatal readmission (28 days)<> Apgar scores<> large for gestational age babies<> breastfeeding initiation<> hospital admission in first 2 years<> development scores (all domains) | Moderate |
| US Baby's First Years | Duncan et al (2025)8 | <> child BMI at age 4<> child health (maternal reported) | Moderate |
| US Baby's First Years | Hart et al (2024)9 | <> language development (age 1-3, maternal report)<> socio-emotional development (age 1-3, maternal report)<> developmental delay concerns (maternal report, age 3)<> early intervention services enrolment (age 2-3) | Moderate |
| US Baby's First Years | Noble et al (2025)10 | child development outcomes at age 4<> language skills<> executive function<> socio-emotional problems<> pre-literacy skills<> brain activity (gamma band)<> visual processing/spatial perception<> developmental diagnoses (maternal reported) | Moderate |
| US Baby's First Years | Sperber et al (2023)11 | <> children's health (age 1-3) (maternal assessment)<> children's sleep (age 1-3)<> health care utilisation (age 1-3)▲ fresh produce consumption (age 2 only) | Moderate |
| US Baby's First Years | Stilwell et al (2024)12 | ▲ breastfeeding intentions met▲ delayed age at entry to formal childcare<> breastfeeding rates/length | Moderate |
| US Baby's First Years | Troller-Renfree et al (2022)13 | ▲ neurodevelopmental markers at age 1 (proximal outcome linked to later cognitive and language outcomes) | Moderate |
| US Baby's First Years | Troller-Renfree et al (2026)14 | ▲ brain activity associated with attention and self-regulation (age 4)<> neurodevelopmental markers at age 4 (incl. brain activity, frontal brain activity, brain activity patterns) | Moderate |
Table A3: Key policy features of early years cash transfers in high income countries (N=11)
| Policy name | Type of payment | Payment timing | Conditional/Unconditional | Universal/targeted | Amount (GBP equiv. indexed to 2026 values | Country | Timeline |
|---|---|---|---|---|---|---|---|
| UK Health in Pregnancy Grant (HiP) | One off payment | At 25 weeks pregnancy | Conditional – prenatal care | Universal | £190(<£600) | UK | 2009-2011 |
| Australian Baby Bonus (ABB) | One off payment | At birth | Unconditional | Universal | A$3000(£1000-£3000) | Australia | 2004-2014 |
| Poland Baby Bonus (PBB) | One off payment | At birth | Unconditional 2006-2009Conditional (from 2009)– prenatal care during 10th week of gestation | Universal | €262 per birth(<£600) | Poland | 2006-20092009- |
| South Korea Baby Bonus (SKBB) | One off payment | At birth | Unconditional (register birth in district) | Universal by district | Wide range dependent on district/birth order.2015 average payments : US$680 first child;US$926 second child; US$2350 third child(£1000-£3000) | South Korea | 2000-2015 |
| Spain Maternity Bonus (ESMB) | One off payment | At birth | Unconditional | Universal (legal resident for 2 years) | €2500 per birth (tax deduction or cash – mother's choice)(£3001+) | Spain | 2007-2010 |
| Swiss Baby Bonus (CHBB) | One off payment | At birth | Unconditional | Universal - canton resident (11 of 26 cantons) | CHF 1,000–1,500 per child(£1000-£3000) | Switzerland | 1969-2017 |
| US Healthy Pregnancy Program (US HPP) | One off payment | At birth | Conditional - timely prenatal care and regular visits | Targeted to low-income or Medicaid-eligible pregnant women | US$100 given each to mother & midwife(<£600) | US | 1998-2001 |
| US NICU Financial Support, Massachusetts | Weekly payments (x3) | Mothers enrolled after birth - baby in NICU | Unconditional (labelled messaging encouraging skin-to-skin care (STSC), visitation, time with infant) | Targeted – Medicaid-eligible mothers and clinical need | US$200 per week (max $600 for 3 weeks)(<£600) | US | 2017-2018 |
| Manitoba Healthy Baby Prenatal Benefit Program (HBPB) | Monthly payments | From 14 weeks pregnancy until birth | Unconditional | Targeted – low-income families | C$10 to C$81.41 per monthi (sliding scale)(Total <£600) | Canada | 2001- |
| Rx Kids – Flint, Michigan | One off payment mid-pregnancy and monthly payments from birth until age 1 | Mid-pregnancy.From birth to age 1. | Unconditional | Universal (in Flint, Michigan) | US$1500 mid pregnancy, US$500 monthly from birth to age 1 (12 payments)(Total £3001+) | US | 2024-(expanded to other states) |
| US Baby's First Years | Monthly payments | Shortly after birth, for first 76 months of child's life (over 6 years) | Unconditional | Targeted – low-income mothers | High-cash group: US$333/monthLow-cash group: US$20/month(Total £3001+) | US | 2018- |
Sources
Pearce, A. (2019). Pathways to inequalities in child health. Archives of Disease in Childhood, 104(10), 998-1003. doi: 10.1136/archdischild-2018-314808
Academy of Medical Sciences. (2024). Prioritising Early Childhood to Promote the Nation’s Health, Wellbeing and Prosperity. Retrieved from <a href="https://acmedsci.ac.uk/policy/policy-projects/child-health" target="_blank">https://acmedsci.ac.uk/policy/policy-projects/child-health</a>
Dundas, R., & Leyland, A. (2022). Investing in early years to reduce non-communicable diseases in adults. European Journal of Public Health, 32(2), 174-175. doi: 10.1093/eurpub/ckab203
Academy of Medical Royal Colleges. (2023). Securing Our Healthy Future. Prevention is Better than Cure. Retrieved from <a href="https://www.aomrc.org.uk/wp-content/uploads/2023/09/Securing_our_healthy_future_0923.pdf" target="_blank">https://www.aomrc.org.uk/wp-content/uploads/2023/09/Securing_our_healthy_future_0923.pdf</a>
Marmot, M. (2010). Fair Society, Healthy Lives. The Marmot Review: Strategic Review of Health Inequalities in England post-2010. Retrieved from <a href="https://www.instituteofhealthequity.org/resources-reports/fair-society-healthy-lives-the-marmot-review" target="_blank">https://www.instituteofhealthequity.org/resources-reports/fair-society-healthy-lives-the-marmot-review</a>
Brydon, R., Bin Haseeb, S., Park, G.R., Ziegler, C., Hwang, S.W., Forget, E.L., … Dunn, J.R. (2024). The effect of cash transfers on health in high-income countries: a scoping review. Social Science & Medicine, 362, 117397. doi: 10.1016/j.socscimed.2024.117397
Candelora, F., Maritano, S., Pizzi, C., Richiardi, M., Richiardi, L., & Boccia, D. (2025). The impact of income support interventions on children’s long-term health trajectories: a systematic review. BMC Public Health, 25(1), 4162. doi: 10.1186/s12889-025-25020-0
Boccia, D., Maritano, S., Pizzi , C., Richiardi, M.G., Lioret, S., & Richiardi, L. (2023). The impact of income-support interventions on life course risk factors and health outcomes during childhood: a systematic review in high income countries. BMC Public Health, 23(1), 744. doi: 10.1186/s12889-023-15595-x
Cooper, K., & Stewart, K. (2021). Does household income affect children’s outcomes? A systematic review of the evidence. Child Indicators Research, 14, 981-1005. doi: 10.1007/s12187-020-09782-0
Gibson, M., Hearty, W., & Craig, P. (2020). The public health effects of interventions similar to basic income: a scoping review. Lancet Public Health, 5(3), 165-176. doi: 10.1016/s2468-2667(20)30005-0
Siddiqi, A., Rajaram, A., & Miller, S.P. (2018). Do cash transfer programmes yield better health in the first year of life? A systematic review linking low-income/middle-income and high-income contexts. Archives of Disease in Childhood, 103(10), 920-926. doi: 10.1136/archdischild-2017-314301
Lisboa, C.S., Guimarães, N.S., Ferreira, A.J.F., da Silva, K.B.B., Alves, F.J.O., Rocha, A.D.S., … Barreto, M.L. (2023). Impact of cash transfer programs on birth and child growth outcomes: systematic review. Ciencia e Saude Coletiva, 28(8), 2417-2432. doi: 10.1590/1413-81232023288.14082022
Hoynes, H., Miller, D., & Simon, D. (2015). Income, the Earned Income Tax Credit, and infant health. American Economic Journal: Economic Policy, 7(1), 172-211. doi: 10.1257/pol.20120179
Bustos, B., Lopez, M., Dodge, K.A., Lansford, J.E., Copeland, W.E., Odgers, C.L., … Bruckner, T.A. (2024). Family cash transfers in childhood and birthing persons and birth outcomes later in life. SSM - Population Health, 25, 101623. doi: 10.1016/j.ssmph.2024.101623
Chung, W., Ha, H., & Kim, B. (2016). Money transfer and birth weight: evidence from the Alaska Permanent Fund Dividend. Economic Inquiry, 54(1), 576-590. doi: 10.1111/ecin.12235
Margerison, C.E., Pilkauskas, N.V., Joachim, G., Luo, Z., & Bruckner, T. (2025). Impacts of the 2021 child tax credit advance monthly payments on birth outcomes in the United States: a natural experiment. American Journal of Epidemiology, 194(2), 3646-3653. doi: 10.1093/aje/kwaf211
Milligan, K., & Stabile, M. (2011). Do child tax benefits affect the well-being of children? Evidence from Canadian Child Benefit expansions. American Economic Journal: Economic Policy, 3(3), 175-205. doi: 10.1257/pol.3.3.175
Hanneke, R., & Brunskill, A. (2024). Searching for the social determinants of health: observations from evidence synthesis publications. Systematic Reviews, 13(1), 134. doi: 10.1186/s13643-024-02551-y
Scottish Government. (2020). Best Start Grant: Interim Evaluation. Retrieved from <a href="https://www.gov.scot/publications/interim-evaluation-best-start-grant/" target="_blank">https://www.gov.scot/publications/interim-evaluation-best-start-grant/</a>
Scottish Government. (2025). Five Family Payments: Evaluation. Retrieved from <a href="https://www.gov.scot/publications/evaluation-five-family-payments/" target="_blank">https://www.gov.scot/publications/evaluation-five-family-payments/</a>
HM Treasury. (2003). Every Child Matters. Retrieved from <a href="https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/272064/5860.pdf" target="_blank">https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/272064/5860.pdf</a>
Scottish Government. (2006). Getting it Right for Every Child (GIRFEC). Retrieved from <a href="https://www.gov.scot/policies/girfec/" target="_blank">https://www.gov.scot/policies/girfec/</a>
Department for Education. (2025). Giving Every Child the Best Start in Life. Retrieved from <a href="https://www.gov.uk/government/publications/giving-every-child-the-best-start-in-life?mc_cid=345ac013b7&mc_eid=d0c9055051" target="_blank">https://www.gov.uk/government/publications/giving-every-child-the-best-start-in-life?mc_cid=345ac013b7&mc_eid=d0c9055051</a>
Scottish Government. (2022). Getting it Right for Every Child (GIRFEC). Policy Statement. Retrieved from <a href="https://www.gov.scot/publications/getting-right-child-girfec-policy-statement/documents/" target="_blank">https://www.gov.scot/publications/getting-right-child-girfec-policy-statement/documents/</a>
Stewart, E. (2022). Welfare Grants in Pregnancy and Early Childhood. MatCHNet Policy Report 1, University of Glasgow. Retrieved from <a href="https://eprints.gla.ac.uk/270469/" target="_blank">https://eprints.gla.ac.uk/270469/</a>
Organisation for Economic Co-operation and Development. (2025). OECD Family Database. Public Spending on Family Benefits. Retrieved from <a href="https://webfs.oecd.org/Els-com/Family_Database/PF1_1_Public_spending_on_family_benefits.pdf" target="_blank">https://webfs.oecd.org/Els-com/Family_Database/PF1_1_Public_spending_on_family_benefits.pdf</a>
Reader, M. (2023). The infant health effects of starting universal child benefits in pregnancy: Evidence from England and Wales. Journal of Health Economics, 89, 102751. doi: 10.1016/j.jhealeco.2023.102751
González, L., & Trommlerová, S. (2022). Cash transfers before pregnancy and infant health. Journal of Health Economics, 83, 102622. doi: 10.1016/j.jhealeco.2022.102622
Kim, W. (2024). Baby bonus, fertility, and missing women. CESifo Working Paper No. 11215. doi: https://ssrn.com/abstract=4908490
Borra, C., Costa-Ramón, A., González, L., & Sevilla, A. (2024). The causal effect of an income shock on children’s human capital. Journal of Labor Economics, 44(2). doi: 10.1086/733052
Gaitz, J., & Schurer, S. (2017). Bonus skills: examining the effect of an unconditional cash transfer on child human capital formation. IZA Discussion Paper No 10525. doi: https://docs.iza.org/dp10525.pdf
Deutscher, N., & Breunig, R. (2018). Baby bonuses: natural experiments in cash transfers, birth timing and child outcomes. Economic Record, 94(304), 1-24. doi: 10.1111/1475-4932.12382
de Gendre, A., Lynch, J., Meunier, A., Pilkington, R., & Schurer, S. (2021). Child health and parental responses to an unconditional cash transfer at birth. IZA Discussion Papers, 14693. doi: https://www.iza.org/publications/dp/14693/child-health-and-parental-responses-to-an-unconditional-cash-transfer-at-birth
Rosenthal, M.B., Li, Z., Robertson, A.D., & Milstein, A. (2009). Impact of financial incentives for prenatal care on birth outcomes and spending. Health Services Research, 44(5), 1465-1479. doi: 10.1111/j.1475-6773.2009.00996.x
Leyland, A.H., Ouédraogo, S., Nam, J., Bond, L., Briggs, A.H., Gray, R., … Dundas, R. (2017). Evaluation of health in pregnancy grants in Scotland: a natural experiment using routine data. Public Health Research, 5(6). doi: 10.3310/phr05060
Adams, J., van der Waal, Z., Rushton, S., & Rankin, J. (2018). Associations between introduction and withdrawal of a financial incentive and timing of attendance for antenatal care and incidence of small for gestational age: natural experimental evaluation using interrupted time series method. BMJ Open, 8(1), 17697. doi: 10.1136/bmjopen-2017-017697
Brownell, M., Chartier, M., Au, W., & Schultz, J. (2010). Evaluation of the Healthy Baby Program. Retrieved from <a href="http://mchp-appserv.cpe.umanitoba.ca/reference/MCHP-Healthy_Baby_Full_Report_WEB.pdf" target="_blank">http://mchp-appserv.cpe.umanitoba.ca/reference/MCHP-Healthy_Baby_Full_Report_WEB.pdf</a>
Brownell, M.D., Chartier, M.J., Nickel, N.C., Chateau, D., Martens, P.J., Sarkar, J., … PATHS Equity for Children Team, . (2016). Unconditional prenatal income supplement and birth outcomes. Pediatrics, 137(6), 20152992. doi: 10.1542/peds.2015-2992
Brownell, M., Nickel, N.C., Chartier, M., Enns, J.E., Chateau, D., Sarkar, J., … Kutz, A. (2018). An unconditional prenatal income supplement reduces population inequities in birth outcomes. Health Affairs, 37(3), 447-455. doi: 10.1377/hlthaff.2017.1290
Enns, J., Nickel, N.C., Chartier, M., Chateau, D., Campbell, R., Phillips-Beck, W., … Brownell, M. (2021). An unconditional prenatal income supplement is associated with improved birth and early childhood outcomes among First Nations children in Manitoba, Canada: a population-based cohort study. BMC Pregnancy and Childbirth, 21(1), 312. doi: 10.1186/s12884-021-03782-w
Struck, S., Enns, J.E., Sanguins , J., Chartier, M., Nickel, N.C., Chateau, D., … Brownell, M. (2021). An unconditional prenatal cash benefit is associated with improved birth and early childhood outcomes for Metis families in Manitoba, Canada. Child and Youth Services Review, 121, 105853. doi: 10.1016/j.childyouth.2020.105853
Hanna, M., Agarwal, S., & Shaefer, L. (2025). Unconditional cash transfers and prenatal care utilization in Flint. JAMA Network Open, 8(10), 2538406. doi: 10.1001/jamanetworkopen.2025.38406
Troller-Renfree , S.V., Costanzo , M.A., Duncan, G.J., Magnuson, K., Gennetian, L.A., Yoshikawa, H., … Noble, K.G. (2022). The impact of a poverty reduction intervention on infant brain activity. Proceedings of the National Academy of Sciences USA, 119(5), 2115649119. doi: 10.1073/pnas.2115649119
Hart, E.R., Gennetian, L.A., Sperber, J.F., Penalva , R., Magnuson, K., Duncan, G.J., … Noble, K.G. (2024). The effect of unconditional cash transfers on maternal assessments of children’s early language and socioemotional development: Experimental evidence from U.S. families residing in poverty. Developmental Psychology. doi: 10.1037/dev0001824
Troller-Renfree, S.V., Costanzo, M.A., Duncan, G.J., Magnuson, K., Gennetian, L.A., Yoshikawa , H., … Noble, K.G. (2026). The impact of a monthly unconditional cash transfer on child brain activity: A 4-year follow-up. Developmental Cognitive Neuroscience, 78, 101673. doi: 10.1016/j.dcn.2026.101673
Noble, K., Magnuson, K., Duncan, G., Gennetian, L.A., Yoshikawa, H., Fox, N.A., … Karhson, D. (2025). The effect of a monthly unconditional cash transfer on children’s development at four years of age: a randomized controlled trial in the U.S. NBER Working Paper 33844. doi: https://www.nber.org/papers/w33844
Sperber, J.F., Gennetian, L.A., Hart, E.R., Kunin-Batson, A., Magnuson, K., Duncan, G.J., … Noble, K.G. (2023). Unconditional cash transfers and maternal assessments of children's health, nutrition, and sleep: a randomized clinical trial. JAMA Network Open, 6(9), 2335237. doi: 10.1001/jamanetworkopen.2023.35237
Chuard, C., & Chuard-Keller, P. (2021). Baby bonus in Switzerland: effects on fertility, newborn health, and birth-scheduling. Health Economics, 30(9), 2092-2123. doi: 10.1002/hec.4366
Courtin, E., Kim, S., Song, S., Yu, W., & Muennig, P. (2020). Can social policies improve health? A systematic review and meta-analysis of 38 randomized trials. The Millbank Quarterly. doi: 10.1111/1468-0009.12451
Fuller, A.E., Zaffar, N., Cohen, E., Pentland, M., Siddiqi, A., Vandermorris, A., … de Oliveira, C. (2022). Cash transfer programs and child health and family economic outcomes: a systematic review. Can J Public Health, 113(3), 433-445. doi: 10.17269/s41997-022-00610-2
Zaneva, M., Guzman-Holst, C., Reeves, A., & Bowes, L. (2022). The impact of monetary poverty alleviation programs on children’s and adolescents’ mental health: a systematic review and meta-analysis across low-, middle-, and high-income countries. Journal of Adolescent Health, 71(2), 147-156. doi: 10.1016/j.jadohealth.2022.02.011
Nishimura, H.M., Snguon, S., Moen, M., & Dean, L.T. (2025). Guaranteed income and health in the United States and Canada: a scoping review. Epidemiologic Reviews, 47(1). doi: 10.1093/epirev/mxaf003
Choudhry, S.A., Brédy, G.S., Cruise, C., Hinds, Q., McConnell, M.A., Agarwal, S., … Murray Horwitz, M.E. (2025). Associations between unconditional cash transfers and postpartum outcomes in the United States : a systematic review. Annals of Internal Medicine, 178(7), 1000-1011. doi: 10.7326/annals-24-03495
Shah, H., & Gennetian, L.A. (2024). Unconditional cash transfers for families with children in the U.S.: a scoping review. Review of Economics of the Household, 22, 415-450. doi: 10.1007/s11150-023-09672-8
Stewart, E., Pearce, A., Given, J., Gilbert, R., Brophy, S., Cookson, R., … Dundas, R. (2023). Identifying opportunities for upstream evaluations relevant to child and maternal health: a UK policy-mapping review. Archives of Disease in Childhood, 108(7), 556-562. doi: 10.1136/archdischild-2022-325219
Barker, T., Habibi, N., Aromataris, E., Stone, J., Leonardi-Bee, J., Sears, K., … Munn, Z. (2024). The revised JBI critical appraisal tool for the assessment of risk of bias for quasi-experimental studies. JBI Evidence Synthesis, 22(3), 378-388. doi: 10.11124/JBIES-23-00268
Barker, T., Stone, J., Sears, K., Klugar, M., Tufanaru, C., Leonardi-Bee, J., … Munn, Z. (2023). The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evidence Synthesis, 21(3), 494-506. doi: 10.11124/JBIES-22-00430
Joanna Briggs Institute. (2020). JBI critical appraisal checklist for cohort studies. Retrieved from <a href="https://jbi.global/sites/default/files/2021-10/Checklist_for_Cohort_Studies.docx" target="_blank">https://jbi.global/sites/default/files/2021-10/Checklist_for_Cohort_Studies.docx</a>
Cygan-Rehm, K., & Karbownik, K. (2022). The effects of incentivizing early prenatal care on infant health. Journal of Health Economics, 83, 102612. doi: 10.1016/j.jhealeco.2022.102612
Andrews, K.G., Martin, M.W., Shenberger, E., Pereira, S., Fink, G., & McConnell, M. (2020). Financial support to medicaid-eligible mothers increases caregiving for preterm infants. Maternal and Child Health Journal, 24(5), 587-600. doi: 10.1007/s10995-020-02905-7
Enns, J.E., Brownell, M., Nickel, N.C., Chartier, M., Chateau, D., Sarkar, J., … Owczar, H. (2025). Birth and early childhood outcomes in families receiving an unconditional prenatal cash benefit. JAMA Network Open, 8(8), 2526996. doi: 10.1001/jamanetworkopen.2025.26996
Duncan, G.J., Magnuson, K., Kunin-Batson, A.S., Fox, N.A., Halpern-Meekin, S., Ainsworth, N.J., … Noble, K.G. (2025). Cash transfers and their effect on maternal and young children’s health: a randomized clinical trial. JAMA Pediatrics, 179(8), 867-875. doi: 10.1001/jamapediatrics.2025.1612
Stilwell, L., Morales-Gracia, M., Magnuson, K., Gennetian, L.A., Sauval, M., Fox, N.A., … Noble, K.G. (2024). Unconditional cash and breastfeeding, child care, and maternal employment among families with young children residing in poverty. Social Service Review, 98(2), 260-292. doi: 10.1086/729364